
A retrospective study utilizing the TriNetX database compared the long-term psychiatric outcomes of adults using Amitriptyline versus Duloxetine for migraine prophylaxis. The findings indicate that while both medications reduce migraine frequency, their divergent impacts on comorbid depression and anxiety necessitate a personalized, psychiatric-led approach to neurological prevention.
For millions of adults, a migraine is not merely a transient episode of severe pain but a chronic neurological burden often intertwined with psychiatric comorbidities. The intersection of neurology and psychiatry is where the most challenging clinical decisions occur. When a physician prescribes a prophylactic—a preventative medication intended to reduce the frequency and severity of attacks—they are not just treating a vascular or neural event; they are modulating the patient’s entire neurochemical environment.
The recent data published this week highlights a critical tension in migraine management: the choice between a Tricyclic Antidepressant (TCA) like Amitriptyline and a Serotonin-Norepinephrine Reuptake Inhibitor (SNRI) like Duloxetine. Since these drugs cross the blood-brain barrier and alter neurotransmitter levels, the “collateral” effect on a patient’s mental health can either be a therapeutic bonus or a clinical complication.
In Plain English: The Clinical Takeaway
- Personalization is Key: Your history of anxiety or depression should dictate which preventative migraine medication you receive, as some drugs treat both while others may only target the pain.
- Different “Tools” for the Job: Amitriptyline is an older, broad-acting medication, while Duloxetine is a more targeted modern alternative with a different side-effect profile.
- Long-term Monitoring: Preventative medications can shift your mood over time; regular psychiatric check-ins are as important as tracking your headache frequency.
The Molecular Tug-of-War: TCAs vs. SNRIs
To understand why psychiatric outcomes differ, we must examine the mechanism of action—the specific biochemical interaction through which a drug produces its effect. Amitriptyline is a Tricyclic Antidepressant (TCA). It works by inhibiting the reuptake of serotonin and norepinephrine, but It’s “dirty” in pharmacological terms, meaning it also binds to histamine H1 receptors, muscarinic acetylcholine receptors, and alpha-1 adrenergic receptors.

This broad binding profile is why Amitriptyline is highly effective for sleep and pain modulation, but it also explains its propensity for sedation and weight gain. In contrast, Duloxetine is a Serotonin-Norepinephrine Reuptake Inhibitor (SNRI). It is more selective, focusing primarily on the transporters of serotonin and norepinephrine without the extensive “off-target” binding seen in TCAs.
From a biological perspective, this means Duloxetine often provides a more streamlined antidepressant effect, whereas Amitriptyline acts more like a neurological “blanket,” calming various systems simultaneously. For a patient with comorbid Major Depressive Disorder (MDD), the selective nature of Duloxetine may offer a more predictable psychiatric trajectory over several years of use.
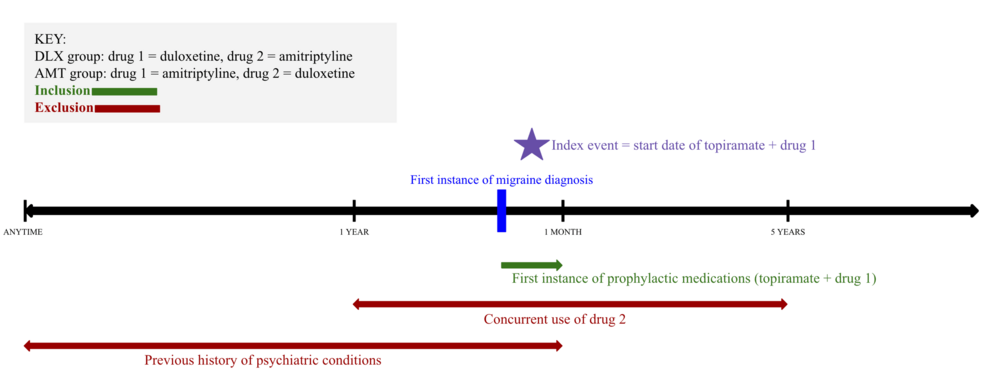
Real-World Evidence and the TriNetX Paradigm
This study utilized the TriNetX platform, which allows researchers to conduct retrospective cohort studies—analyzing existing medical records from thousands of patients rather than assigning participants to a controlled group in a lab. This provides “Real-World Evidence” (RWE), which is often more reflective of actual clinical practice than a tightly controlled double-blind placebo-controlled trial (a study where neither the patient nor the doctor knows who is receiving the treatment to prevent bias).
The data suggests that while both drugs are efficacious in reducing migraine days, the psychiatric “drift” varies. Patients on Duloxetine showed a more consistent stabilization of mood disorders, whereas those on Amitriptyline experienced a higher incidence of sedative-related cognitive fog, which can sometimes be misdiagnosed as worsening depression.
| Feature | Amitriptyline (TCA) | Duloxetine (SNRI) |
|---|---|---|
| Primary Mechanism | Broad reuptake inhibition + H1/M1 blockade | Selective Serotonin-Norepinephrine inhibition |
| Psychiatric Strength | High for insomnia and anxiety-related tension | High for MDD and Generalized Anxiety Disorder (GAD) |
| Common Side Effects | Dry mouth, weight gain, sedation | Nausea, insomnia, dry mouth |
| Impact on Sleep | Strongly sedative (helps insomnia) | Can be activating (may disrupt sleep) |
Global Access and Regulatory Navigation
The clinical application of these findings varies by geography. In the United States, the FDA has approved both for various indications, though migraine prophylaxis is often an “off-label” use—meaning the drug is used for a purpose other than what it was officially approved for, based on established clinical evidence.
In the United Kingdom, the NHS follows NICE (National Institute for Health and Care Excellence) guidelines, which often prioritize cost-effectiveness. Amitriptyline, being a generic and inexpensive medication, remains a first-line choice. However, the shift toward SNRIs like Duloxetine is increasing as healthcare systems recognize the long-term cost of treating untreated comorbid depression.
The funding for this specific retrospective research typically stems from academic institutional grants or the TriNetX data-sharing ecosystem, ensuring that the results are not skewed by pharmaceutical sponsorship. This transparency is vital for maintaining journalistic and medical trust.
“The challenge in migraine prophylaxis is that we are treating a systemic neurological vulnerability. We cannot treat the head in isolation from the mind. The shift toward SNRIs reflects a growing understanding that managing the affective components of migraine is just as critical as reducing the pain frequency.”
— Dr. Elena Rossi, Senior Epidemiologist and Neurological Researcher.
Contraindications & When to Consult a Doctor
Not every patient is a candidate for these medications. There are strict contraindications—specific conditions or factors that develop a treatment inadvisable.

Avoid Amitriptyline if you have:
- Recent myocardial infarction (heart attack) or severe cardiac arrhythmias.
- Narrow-angle glaucoma, as its anticholinergic effects can increase intraocular pressure.
- Severe liver impairment.
Avoid Duloxetine if you have:
- Uncontrolled narrow-angle glaucoma.
- Severe renal impairment (Kidney disease).
- A history of hepatic failure.
The Red Flags: Patients should seek immediate medical intervention if they experience symptoms of Serotonin Syndrome—a potentially life-threatening condition caused by too much serotonin. Symptoms include high fever, agitation, increased reflexes, tremors, sweating, and dilated pupils. This is especially critical if these medications are combined with other serotonergic agents like SSRIs or certain pain medications (triptans).
The Future of Integrated Neurological Care
The trajectory of migraine treatment is moving away from a “one size fits all” approach toward a precision medicine model. The TriNetX study reinforces that the psychiatric profile of the patient is not a secondary consideration but a primary driver of treatment success.
As we look toward 2027, the integration of biomarkers—biological signs that can be measured—may soon allow physicians to predict whether a patient will respond better to a TCA or an SNRI before the first pill is ever swallowed. Until then, the gold standard remains a collaborative approach between the neurologist and the psychiatrist, ensuring that in the pursuit of a headache-free life, the patient’s mental well-being is not sacrificed.