
Anterolateral bowing of the tibia is a rare skeletal deformity characterized by an outward and forward curvature of the shinbone. A recent cadaveric case report published in Cureus utilizes histopathological correlation to analyze how bone remodeling and structural anomalies contribute to this specific misalignment, providing critical insights for orthopedic surgical planning.
For the average person, a slight curve in the leg might seem like a cosmetic quirk. However, for clinicians, this bowing represents a complex interplay of mechanical stress and biological failure. When the tibia—the primary weight-bearing bone of the lower leg—deviates from its vertical axis, it alters the distribution of force across the knee and ankle joints. This isn’t just about alignment; it’s about the long-term integrity of the cartilage and the prevention of premature osteoarthritis.
In Plain English: The Clinical Takeaway
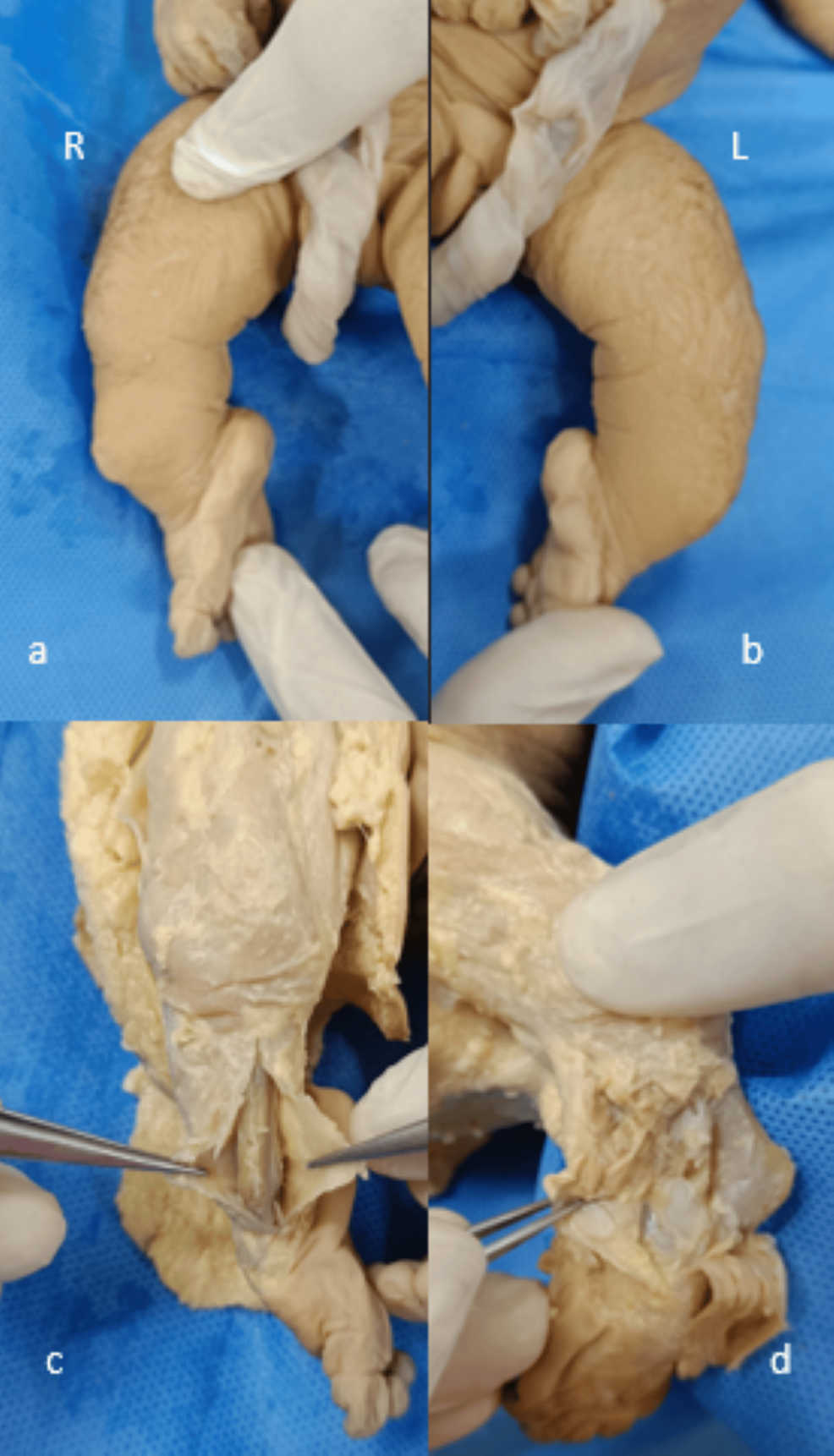
- What happened: Researchers studied a deceased donor’s leg to see exactly why the shinbone bowed outward and forward.
- The finding: The bowing wasn’t just a shape issue; the microscopic structure of the bone (histopathology) showed changes in how the bone handles pressure.
- Why it matters: Understanding these patterns helps surgeons better align implants during knee or ankle replacements in living patients.
The Cellular Mechanics of Tibial Deformity
The core of this case report lies in the mechanism of action—the specific biological process—of bone remodeling. In a healthy tibia, bone is constantly broken down and rebuilt to withstand the stresses of walking. When this process is disrupted, we see a failure in “Wolff’s Law,” the principle that bone grows and remodels in response to the forces placed upon it.
The “anterolateral” aspect refers to the front (anterior) and outer (lateral) side of the bone. Histopathological correlation—the process of matching microscopic tissue samples with the visible physical deformity—revealed that the bowing was not merely a result of external pressure, but a structural inadequacy in the cortical bone. The cortical bone is the dense, hard outer shell that provides the leg’s primary strength. In this case, the thinning of this shell in specific zones allowed the bone to yield to mechanical loads, resulting in a permanent curve.
This level of detail is crucial because it distinguishes between congenital deformities (present at birth) and acquired deformities, such as those caused by Rickets or Paget’s disease. According to the PubMed database, metabolic bone diseases often manifest as similar bowing, but the histopathological markers differ significantly from purely mechanical bowing.
Comparing Tibial Bowing Patterns and Clinical Impacts
To understand how anterolateral bowing differs from more common deformities, we must look at the axis of deviation. Most common bowing, such as genu varum (bow-legs), occurs in a single plane. Anterolateral bowing is more complex because it involves a rotational component, affecting both the frontal and sagittal planes of the body.

| Deformity Type | Primary Plane of Bowing | Primary Structural Cause | Joint Impact |
|---|---|---|---|
| Genu Varum | Frontal (Lateral) | Medial compartment overload | Medial knee arthritis |
| Anterolateral Bowing | Combined Frontal/Sagittal | Cortical thinning/Remodeling failure | Multi-axial joint instability |
| Genu Valgum | Frontal (Medial) | Lateral compartment overload | Lateral knee arthritis |
Global Orthopedic Implications and Regulatory Standards
The findings from this cadaveric study have direct implications for how the FDA in the United States and the EMA in Europe regulate the design of orthopedic implants. Most standard tibial trays used in Total Knee Arthroplasty (TKA) are designed for a relatively straight bone. When a surgeon encounters a patient with significant anterolateral bowing, a “standard” implant may not fit the anatomy, leading to poor implant stability or premature loosening.
In the UK, the NHS often utilizes specialized “patient-specific instrumentation” (PSI) for complex deformities. This involves using 3D printing and CT scans to create guides tailored to the patient’s unique bow. By correlating the histopathology of the bone with the physical curve, researchers can help engineers develop implants that account for the reduced bone density often found on the concave side of the bow.
The research was published via Cureus, a journal that utilizes a peer-review model focused on rapid dissemination of clinical case reports. While this specific study was a case report (meaning it focused on one individual) rather than a double-blind placebo-controlled trial (a gold-standard study where neither the patient nor the researcher knows who received the treatment), it provides the “proof of concept” necessary to trigger larger epidemiological studies.
Contraindications & When to Consult a Doctor
It is vital to distinguish between a natural, slight curvature of the limb and a pathological deformity. You should seek a professional orthopedic evaluation if you experience the following:
- Asymmetrical Limb Length: If one leg appears significantly shorter or more curved than the other.
- Localized Bone Pain: Persistent aching in the shin that worsens with weight-bearing activity.
- Joint Instability: A feeling that the knee or ankle is “giving way” during normal gait.
- Rapid Change: Any noticeable increase in the curvature of the leg over a short period.
Medical intervention, such as corrective osteotomy (surgically breaking and resetting the bone), is generally contraindicated in patients with severe osteoporosis or uncontrolled diabetes, as these conditions significantly impair the bone’s ability to heal and fuse.
The Future of Precision Alignment
The shift toward “personalized orthopedics” depends on these rare case reports. By mapping the histopathological correlation of the tibia, medicine moves away from a one-size-fits-all approach. The goal is to move toward a future where the biological density of the bone dictates the surgical approach, ensuring that implants are anchored in the strongest possible tissue.
References
- Cureus Journal of Medical Science – Cadaveric Case Report of Anterolateral Bowing of Tibia With Histopathological Correlation.
- World Health Organization (WHO) – Musculoskeletal Health Guidelines.
- Centers for Disease Control and Prevention (CDC) – Bone Health and Osteoporosis Data.
- The Lancet – Orthopedic Surgery and Implant Stability Research.