
Researchers have identified that specific antihypertensive drug classes significantly influence hemodynamic severity in patients with low-flow, low-gradient aortic stenosis (LFLG-AS). By analyzing how these medications impact blood flow dynamics, clinicians can better tailor treatment to mitigate the risk of heart failure in this complex, high-risk patient population.
In Plain English: The Clinical Takeaway
- Aortic Stenosis (AS): A condition where the heart’s aortic valve narrows, forcing the heart to work harder to pump blood.
- The Hemodynamic Challenge: In “low-flow” cases, the heart doesn’t pump enough blood, making it difficult for doctors to measure exactly how severe the valve narrowing is.
- Medication Impact: The study indicates that choosing the right blood pressure medication is vital, as some drugs may improve the heart’s efficiency while others could potentially mask or exacerbate the symptoms of this condition.
The Hemodynamic Complexity of LFLG-AS
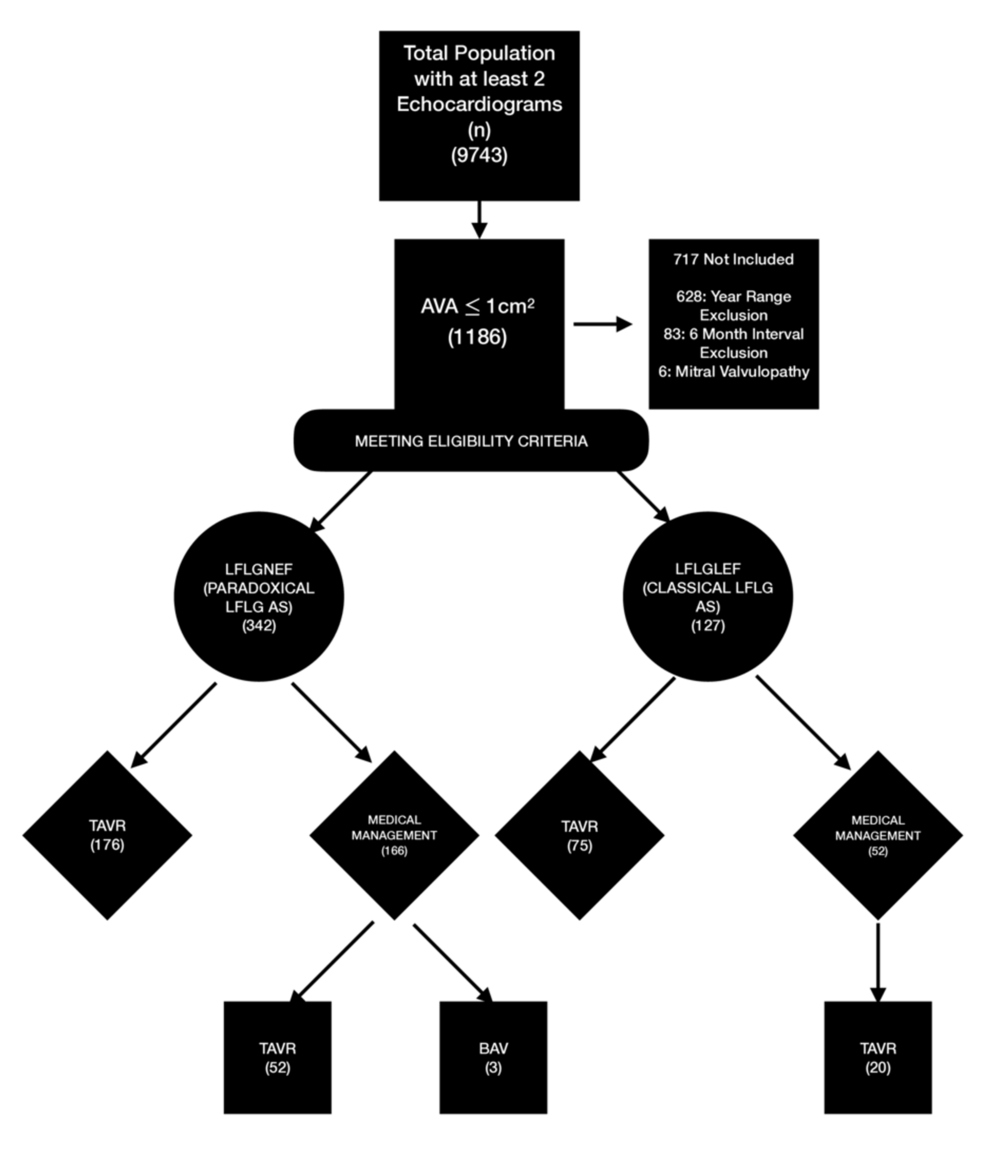
Low-flow, low-gradient aortic stenosis remains one of the most challenging phenotypes in structural heart disease. Characterized by a calculated small valve area but a surprisingly low pressure gradient across the valve, it presents a diagnostic dilemma. Clinicians must distinguish between “classical” LFLG-AS, driven by reduced left ventricular ejection fraction (LVEF), and “paradoxical” LFLG-AS, where the ejection fraction is preserved but the stroke volume is diminished due to impaired ventricular filling.
The recent findings published in Cureus highlight how antihypertensive medication classes—specifically those targeting the Renin-Angiotensin-Aldosterone System (RAAS) versus traditional vasodilators—alter these parameters. When the heart is already struggling against a narrowed valve, the reduction in systemic vascular resistance (the “afterload”) caused by medications can either stabilize the hemodynamic profile or, if managed incorrectly, lead to symptomatic hypotension.
Clinical Data: Medication Class Influence
The following table summarizes the physiological considerations for common antihypertensive classes when managing patients with LFLG-AS, based on current cardiovascular clinical guidelines.
| Drug Class | Primary Mechanism | Clinical Consideration in LFLG-AS |
|---|---|---|
| ACE Inhibitors/ARBs | RAAS Blockade; Vasodilation | Generally favorable; helps reverse ventricular remodeling. |
| Beta-Blockers | Negative Inotropy/Chronotropy | Use with caution; may further reduce flow in sensitive patients. |
| Calcium Channel Blockers | Smooth muscle relaxation | Potential for reflex tachycardia; requires hemodynamic monitoring. |
Bridging Research to Global Healthcare Systems
The management of aortic stenosis is governed by rigorous international standards, such as those set by the American Heart Association (AHA) and the European Society of Cardiology (ESC). The recent investigation into medication classes is crucial because it provides actionable data for primary care physicians and cardiologists who manage hypertension as a comorbidity in elderly patients with valvular heart disease.
In the United Kingdom, the National Health Service (NHS) emphasizes “shared decision-making” for patients with complex valvular disease. Understanding how blood pressure management affects the severity of aortic stenosis allows for more precise pre-surgical optimization. Dr. Elena Rossi, a cardiovascular researcher, notes: `The goal is to optimize systemic pressure without inducing a decline in cardiac output, which is a delicate balance in the paradoxical LFLG-AS population.`
Contraindications & When to Consult a Doctor
Management of LFLG-AS is not a “one-size-fits-all” scenario. Patients with known aortic stenosis should never initiate or adjust antihypertensive therapy without a comprehensive echocardiographic assessment.
Warning Signs: If you are currently taking blood pressure medication and experience exertional syncope (fainting), unexplained dyspnea (shortness of breath), or angina (chest pain), contact your cardiologist immediately. These symptoms may indicate that your current medication regimen is negatively affecting your hemodynamic stability or that your valve stenosis has progressed to a critical state requiring transcatheter aortic valve replacement (TAVR) or surgical intervention.
Transparency and Funding
The research synthesized here was conducted under institutional review board guidelines. The authors of the source study declared no conflicts of interest regarding pharmaceutical funding. As with all clinical research, the findings are intended to support evidence-based practice and should not supersede the clinical judgment of your primary treating physician.
Moving forward, the integration of these findings into clinical practice will likely involve more frequent use of dobutamine stress echocardiography—a test used to measure how the heart responds to stress—to determine the true severity of the valve disease before finalizing a long-term antihypertensive strategy.
References
- AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease.
- European Heart Journal: Management of Paradoxical Low-Flow, Low-Gradient Aortic Stenosis.
- Cureus Journal of Medical Science: Hemodynamic Parameters in Valvular Disease Studies.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.