
Diagnostic Precision and the Economics of Breast Cancer Care
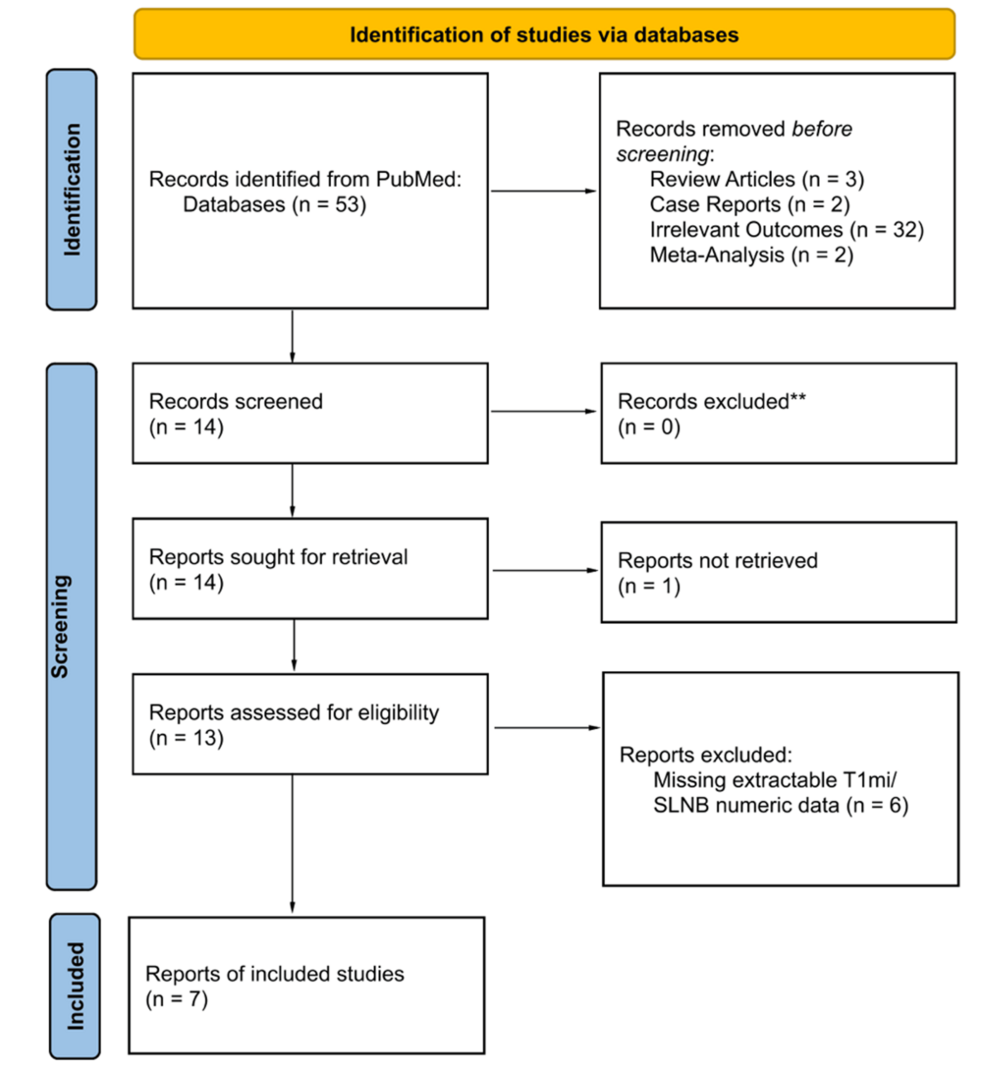
Microinvasive breast cancer, defined by tumor invasion of the stroma measuring 1 mm or less, presents a complex clinical management challenge that directly influences hospital resource allocation and insurance reimbursement models. A recent systematic review and meta-analysis published in Cureus indicates that axillary nodal involvement in these cases occurs in approximately 1.7% to 2.4% of patients, challenging the necessity of routine sentinel lymph node biopsy (SLNB) in early-stage surgical interventions.
The Bottom Line
- Surgical De-escalation: The low incidence of nodal positivity suggests that routine SLNB may be medically unnecessary for many microinvasive patients, providing an opportunity to reduce hospital procedural costs.
- Resource Optimization: By shifting toward less invasive diagnostic protocols, healthcare systems can reduce operating room time and pathology overheads, which currently account for a significant portion of oncology-related hospital expenditures.
- Insurance Implications: Payers are increasingly scrutinizing “standard of care” procedures that yield low diagnostic utility; findings like these provide the actuarial evidence needed to adjust coverage policies for surgical oncology.
The Financial Burden of Over-Diagnosis
When markets analyze the oncology sector, the focus is often on high-cost pharmaceutical pipelines from giants like Merck (NYSE: MRK) or Roche (SWX: ROG). However, the operational side of oncology—specifically surgical procedures—represents a massive, often overlooked, segment of healthcare spending. The standard practice of performing SLNB in microinvasive breast cancer involves anesthesia, surgical time, and specialized pathology services.
According to data reported by the American Hospital Association, the average cost of an outpatient surgical procedure can range from $3,000 to $10,000 depending on the facility and region. If 2.4% or fewer patients exhibit nodal involvement, the “cost per positive finding” in a routine screening model becomes inefficient. For hospital networks managing oncology centers, these findings suggest a pivot toward value-based care models where clinical outcomes are decoupled from procedural volume.
Market-Bridging: The Shift Toward Value-Based Oncology
The broader diagnostic market, including firms like Hologic (NASDAQ: HOLX) and Exact Sciences (NASDAQ: EXAS), is currently navigating a shift where precision diagnostics are prioritized over invasive exploratory surgery. The Cureus study reinforces the economic argument for limiting surgical intervention when the probability of disease spread is statistically negligible.
“The move toward de-escalation in breast cancer surgery is not just a clinical trend; it is a direct response to the rising cost of care and the need for more efficient resource allocation,” notes Dr. Sarah Cannon, a health economist specializing in oncology delivery systems. “When we identify patient cohorts that do not require invasive staging, we effectively lower the total cost of care for the entire population.”
Comparative Analysis of Surgical Protocols
| Metric | Standard SLNB Protocol | De-escalated/Selective Protocol |
|---|---|---|
| Average Procedure Cost | $5,000 – $8,000 | $0 – $500 (Imaging only) |
| Pathology Overhead | High (Frozen sections/IHC) | Minimal |
| Patient Recovery Time | Moderate | Negligible |
| Diagnostic Yield (Nodal Positivity) | 1.7% – 2.4% | N/A |
Institutional Impact and Future Trajectory
For institutional investors, the takeaway is clear: the oncology market is bifurcating. One lane remains focused on high-margin, late-stage systemic therapies, while the other—the diagnostic and surgical lane—is moving toward significant cost-containment.
As healthcare systems face pressure from both the Centers for Medicare & Medicaid Services (CMS) and private insurers to provide evidence-based, cost-effective care, the protocols for microinvasive breast cancer are likely to evolve. We expect to see a tightening of clinical guidelines, which will likely reduce the volume of SLNB procedures. This creates a ripple effect: decreased demand for surgical supplies and specialized pathology services, balanced by an increased demand for high-resolution imaging and molecular diagnostic tools.
The integration of these findings into clinical practice will be gradual, but the economic signal is unambiguous. Hospitals that adopt these de-escalation strategies early will improve their operational efficiency and align themselves with the shifting requirements of value-based reimbursement frameworks. As we move into the next fiscal cycle, expect surgical oncology to be a primary target for internal efficiency audits as providers look to protect margins against inflationary labor and facility costs.
*Disclaimer: The information provided in this article is for educational and informational purposes only and does not constitute financial advice.*