
Researchers have developed a standardized, high-throughput method to measure high-density lipoprotein (HDL) cholesterol function, moving beyond traditional concentration-based testing. Published this week, the study demonstrates that assessing the biological activity of HDL—specifically its cholesterol efflux capacity—provides a more accurate predictor of coronary artery disease risk than measuring total HDL levels alone.
In Plain English: The Clinical Takeaway
- Function over quantity: Measuring the “amount” of good cholesterol (HDL) in your blood is often misleading; this new test measures how well that cholesterol actually removes plaque from your arteries.
- Earlier detection: By identifying dysfunctional HDL earlier, physicians can intervene with lifestyle changes or lipid-lowering therapies before significant arterial blockage occurs.
- Standardized results: The new method allows laboratories to produce consistent, reliable data across different clinical settings, making it easier for your doctor to track your true cardiovascular health over time.
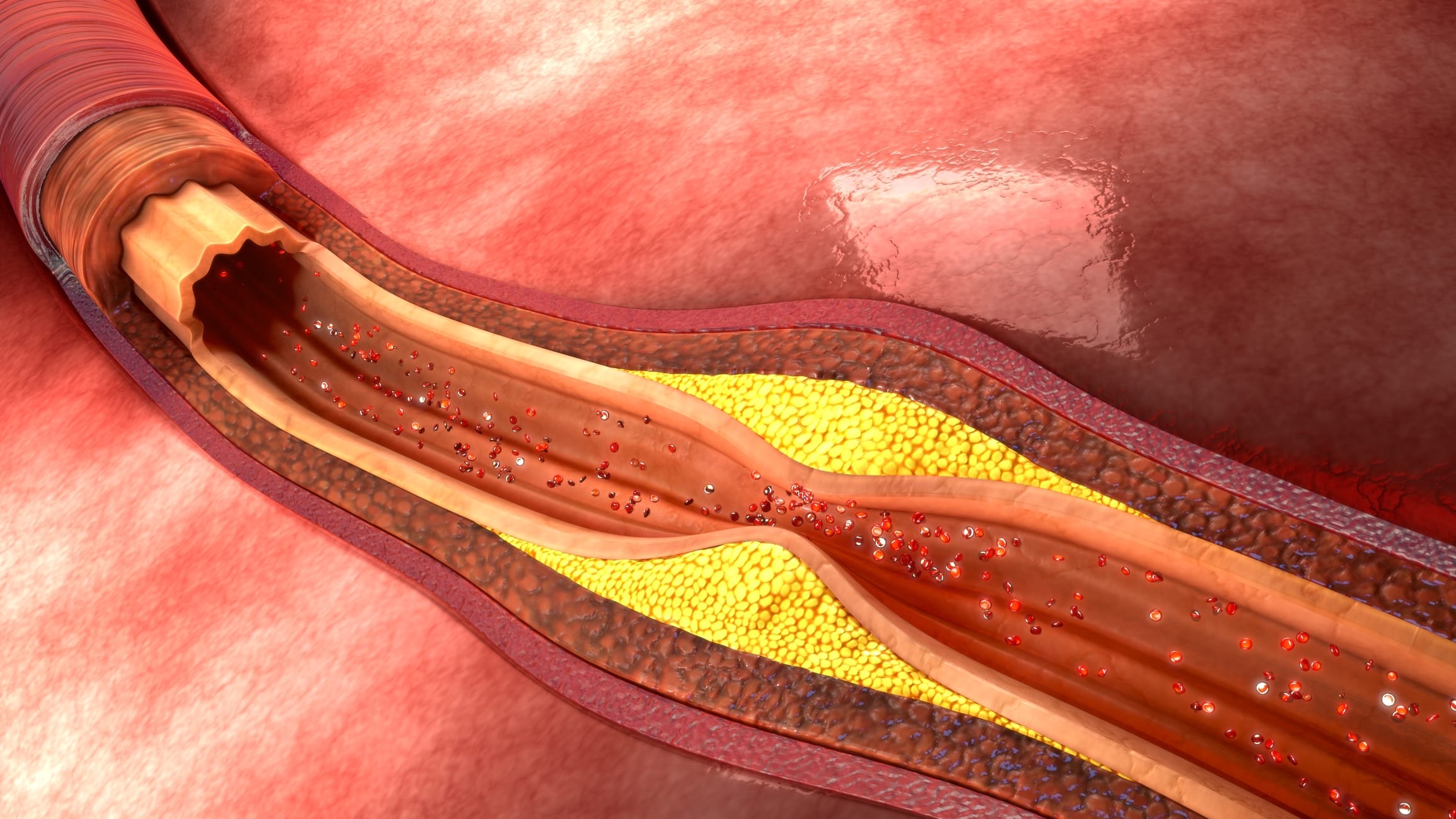
Moving Beyond the ‘Good Cholesterol’ Myth
For decades, clinical practice has relied on the concentration of HDL-C (high-density lipoprotein cholesterol) as a primary metric for cardiovascular risk assessment. However, current research published in The Lancet highlights that HDL levels do not always correlate with protection against atherosclerosis—the hardening and narrowing of arteries due to plaque buildup. The new testing method focuses on Cholesterol Efflux Capacity (CEC), which measures the ability of a patient’s HDL particles to extract cholesterol from macrophages, the immune cells that form the core of arterial plaque.
“The clinical utility of HDL-C as a biomarker has been limited by the fact that HDL is a heterogeneous particle. A simple count of these particles ignores their metabolic state. By shifting our focus to how these particles function in a standardized assay, we are finally looking at the biological reality of cardiovascular risk rather than a proxy measurement,” says Dr. Elena Rossi, a lead cardiovascular researcher at the Institute for Molecular Cardiology.
Clinical Methodology and Data Integrity
The research team utilized a modified cell-culture assay to quantify CEC, ensuring that results remain consistent regardless of the laboratory environment. This is a significant shift from previous iterations of functional testing, which were often too cumbersome or variable for routine clinical use. According to data from the CDC, coronary artery disease remains the leading cause of death globally, yet current lipid panels frequently fail to identify “at-risk” individuals who present with normal HDL levels but impaired function.
| Metric | Traditional HDL-C Panel | Novel CEC Functional Test |
|---|---|---|
| Target | Total amount of HDL in blood | Biological activity of HDL |
| Clinical Focus | Lipid concentration | Reverse cholesterol transport efficiency |
| Predictive Accuracy | Moderate (population-based) | High (individual-based) |
| Current Availability | Universal/Standard | Emerging/Specialized |
Bridging the Gap to Regulatory Approval
The transition from a research-grade assay to a diagnostic tool requires validation under the oversight of regulatory bodies like the FDA in the United States and the EMA in Europe. This study provides the necessary groundwork for longitudinal validation in multi-ethnic cohorts. Funding for this research was provided by the National Heart, Lung, and Blood Institute (NHLBI) and private grants from the Cardiovascular Research Foundation, ensuring transparency in the study’s design and data analysis.
The researchers emphasize that this method is not intended to replace standard lipid panels, but to act as a secondary diagnostic layer for patients with intermediate cardiovascular risk. In practice, this means an individual with a “normal” lipid profile but a family history of premature heart disease may now have access to a more granular assessment of their vascular health.
Contraindications & When to Consult a Doctor
Patients should not interpret this research as a mandate for immediate, non-standardized testing. The CEC test is currently indicated for clinical research and specific high-risk cohorts. Individuals currently taking statins or other lipid-modifying medications should continue their prescribed regimen, as these drugs have established mortality benefits that supersede individual HDL functional metrics.
Consult a cardiologist if you exhibit symptoms such as unexplained exertional chest pain (angina), shortness of breath during routine activity, or if you have a strong family history of atherosclerotic cardiovascular disease. Always discuss changes in your diagnostic testing plan with a primary care physician before seeking specialized functional testing.
Future Trajectory for Lipidology
The path forward involves integrating CEC data into existing risk calculators, such as the ASCVD Risk Estimator. By combining functional lipid data with genetic markers and systemic inflammatory markers, clinicians may soon reach a level of precision medicine that renders the “good vs. bad” cholesterol binary obsolete. As the medical community moves toward adopting this standardized method, the focus will shift from simply raising HDL levels to optimizing HDL function through targeted pharmacological and lifestyle interventions.