
Emergency room surveys reveal significant gaps in measles vaccination coverage and persistent vaccine hesitancy across multiple U.S. States, with California reporting its highest annual case count in seven years as of early 2026, prompting urgent public health reassessment of immunization outreach and access barriers.
Understanding the Measles Resurgence: Beyond Headlines
Despite the measles, mumps, and rubella (MMR) vaccine being over 97% effective with two doses, declining immunization rates in certain communities have eroded herd immunity, which requires approximately 95% coverage to prevent sustained transmission. Measles spreads via airborne respiratory droplets when an infected person coughs or sneezes, and the virus can remain infectious in the air for up to two hours. One dose of MMR vaccine provides about 93% protection, while two doses raise efficacy to 97%, according to the CDC. The virus initially infects respiratory epithelial cells before spreading to lymphoid tissue, causing immunosuppression that can last weeks to months—increasing vulnerability to secondary infections like pneumonia or encephalitis.
In Plain English: The Clinical Takeaway
- Two doses of the MMR vaccine provide nearly complete protection against measles, and gaps in vaccination—even small ones—can quickly lead to outbreaks due to how easily the virus spreads.
- Vaccine hesitancy often stems from misinformation about safety, but extensive research shows the MMR vaccine does not cause autism, a myth thoroughly debunked by large-scale studies involving over a million children.
- If you’re unsure about your vaccination status or have been exposed to measles, contact a healthcare provider promptly; post-exposure prophylaxis with the MMR vaccine or immunoglobulin can prevent illness if given within specific time windows.
Geo-Epidemiological Bridging: State-Level Disparities and System Strain
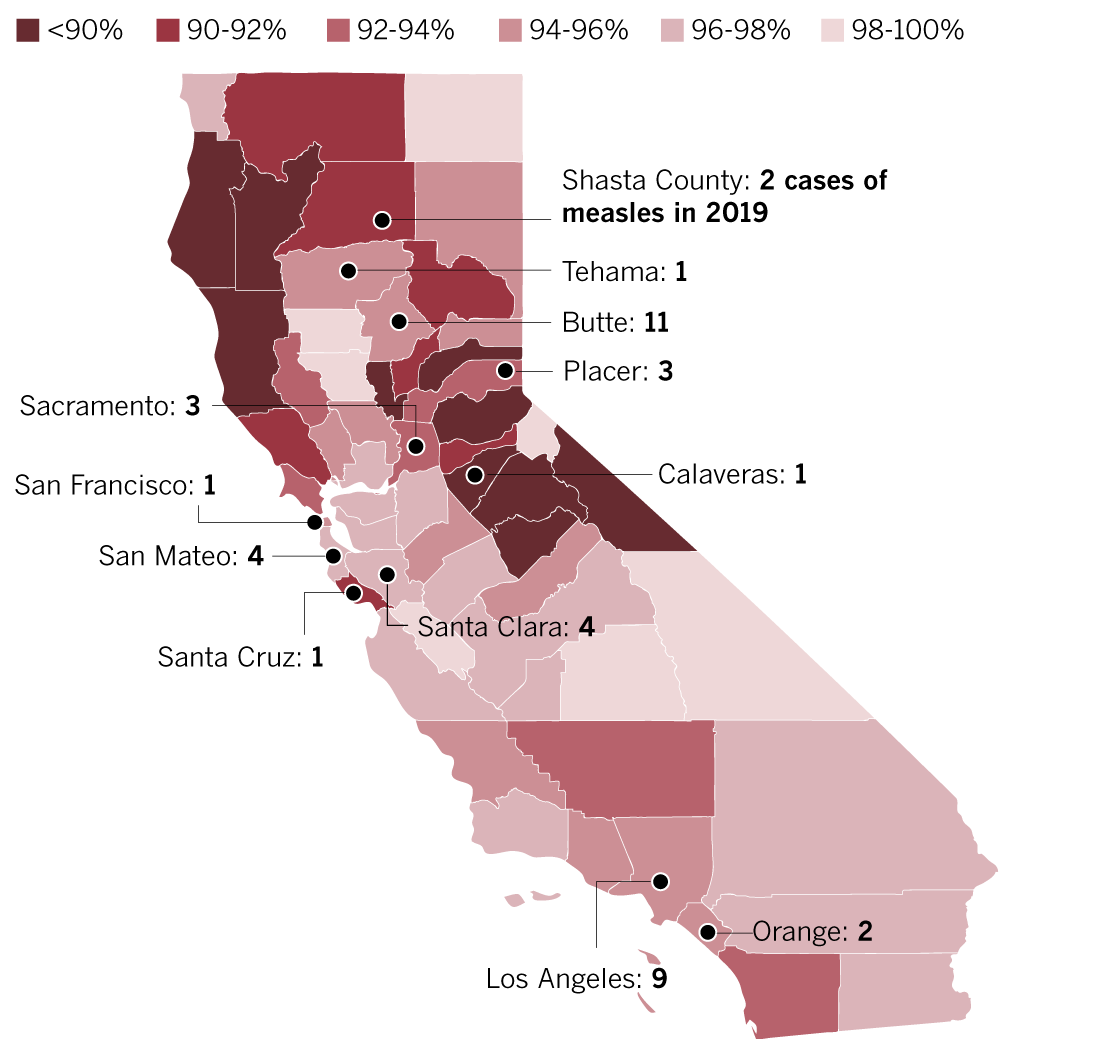
As of April 2026, California has reported over 180 confirmed measles cases—the highest annual total since 2019—with clusters concentrated in Los Angeles County and the Central Valley, according to the California Department of Public Health (CDPH). These outbreaks correlate with regions where kindergarten MMR exemption rates exceed 4.5%, particularly in private and charter schools. In contrast, states like Mississippi and West Virginia, which maintain strict non-medical exemption policies, report sustained MMR coverage above 95% and zero measles cases in 2025–2026. The CDC’s National Immunization Survey-Teen (NIS-Teen) data from 2024 shows national MMR coverage among adolescents aged 13–17 at 89.3%, leaving nearly 1 in 10 inadequately protected. Emergency departments in outbreak-affected areas report increased strain, with fever and rash evaluations consuming significant resources; up to 30% of measles cases require hospitalization, primarily for dehydration or respiratory complications.
Funding, Bias Transparency, and Expert Perspectives
The emergency room survey referenced in recent public health discussions was conducted by researchers at the Johns Hopkins Bloomberg School of Public Health and funded by the Centers for Disease Control and Prevention (CDC) under cooperative agreement U01IP001122, ensuring alignment with federal immunization priorities without industry influence. Dr. Saad Omer, Director of the Yale Institute for Global Health and lead epidemiologist on measles dynamics, emphasized in a March 2026 briefing:
“We’re not seeing vaccine failure—we’re seeing vaccination gaps. The measles virus finds the unvaccinated, and until we close those immunity gaps with equitable access and trust-building, outbreaks will persist.”
Similarly, Dr. Michelle Fiscus, former Tennessee vaccine director and current fellow at the Duke-Margolis Center for Health Policy, noted in a CDC Expert Commentary:
“Hesitancy isn’t monolithic. In some communities, it’s about historical mistrust; in others, it’s logistical—difficulty taking time off work, lack of transportation, or confusion about where to go. We require tailored solutions, not one-size-fits-all mandates.”
Mechanism of Action and Vaccine Science: Clarifying Misconceptions
The MMR vaccine contains live attenuated strains of measles, mumps, and rubella viruses. Upon injection, the weakened measles virus replicates minimally in the body, triggering an adaptive immune response without causing disease. This process activates B cells to produce neutralizing antibodies against the measles hemagglutinin protein and stimulates cytotoxic T cells that eliminate infected cells. The immune system then establishes memory cells capable of mounting a rapid response upon future exposure. Unlike mRNA vaccines, which deliver genetic instructions for antigen production, the MMR vaccine relies on the attenuated virus itself to induce immunity—a well-established platform used safely for over 50 years. Extensive post-licensure monitoring, including Vaccine Safety Datalink (VSD) studies involving millions of doses, confirms no causal link between MMR vaccination and autism spectrum disorder, a conclusion reinforced by a 2019 Danish cohort study of 657,461 children published in Annals of Internal Medicine.
Contraindications & When to Consult a Doctor
- The MMR vaccine is contraindicated in individuals with severe immunodeficiency (e.g., from chemotherapy, congenital disorders like SCID, or high-dose corticosteroids) and those who experienced a life-threatening allergic reaction to a prior dose or vaccine component such as gelatin or neomycin.
- Pregnant individuals should not receive the MMR vaccine due to theoretical fetal risk, though no cases of congenital rubella syndrome have been linked to the vaccine; vaccination is recommended postpartum or before conception.
- Seek immediate medical attention if you or a child develops high fever (>104°F), severe cough, difficulty breathing, or neurological symptoms like confusion or seizures during a suspected measles infection—these may indicate complications such as pneumonia or encephalitis requiring hospitalization.
- If exposed to measles and unvaccinated, consult a healthcare provider within 72 hours; post-exposure MMR vaccination may prevent or modify illness, while immunoglobulin is recommended for high-risk groups (e.g., immunocompromised, infants <6 months) within six days of exposure.
| Metric | Value | Source |
|---|---|---|
| MMR Vaccine Efficacy (2 doses) | 97% | CDC |
| Herd Immunity Threshold for Measles | ~95% | WHO |
| National MMR Coverage (Adolescents 13–17, 2024) | 89.3% | CDC NIS-Teen |
| California Measles Cases (2026 YTD) | 180+ | CDPH |
| Average Hospitalization Rate for Measles | ~30% | Journal of Infectious Diseases |
References
- Centers for Disease Control and Prevention. Measles (Rubeola) Vaccination. Updated 2025.
- World Health Organization. Measles Surveillance Data. 2026.
- California Department of Public Health. Measles Outbreak Reports, 2025–2026.
- Jain, A. Et al. Autism Occurrence by MMR Vaccine Status Among US Children With Older Siblings With Autism. JAMA Pediatrics. 2015;169(8):752–759.
- Hviid, A. Et al. Measles, Mumps, Rubella Vaccination and Autism: A Nationwide Cohort Study. Annals of Internal Medicine. 2019;170(8):513–520.
As measles exploits even minor declines in vaccine coverage, the path forward requires not only scientific clarity but also community-centered engagement. Addressing hesitancy with empathy, strengthening access in underserved areas, and maintaining trust in public health institutions are essential to preventing further erosion of hard-won disease control. The MMR vaccine remains one of the most effective tools in modern medicine—its success now depends on our collective willingness to use it wisely and equitably.