
Rural Americans face higher mortality rates from heart disease, cancer, unintentional injuries, chronic lower respiratory disease, and stroke compared to urban residents. This disparity is driven by systemic barriers to healthcare access, a higher prevalence of behavioral risk factors, and critical shortages of specialized medical providers in non-metropolitan areas.
This mortality gap represents a profound failure in the equitable distribution of healthcare resources. When we analyze the “rural health penalty,” we are looking at a complex intersection of socio-economic determinants—such as lower median incomes and higher smoking rates—and structural deficiencies, including the closure of critical access hospitals. For a patient in a metropolitan hub, a myocardial infarction (heart attack) is a medical emergency; for a patient in a remote county, it is a race against geography where the “Golden Hour”—the critical window for intervention to prevent permanent muscle damage—is often lost to transit time.
In Plain English: The Clinical Takeaway
- Geography is a Risk Factor: Living in a rural area statistically increases your risk of death from the five leading causes of mortality due to slower emergency response times.
- Screening Gaps: Rural patients are less likely to receive early detection for cancers and heart disease, meaning illnesses are often diagnosed at a more advanced, harder-to-treat stage.
- Preventable Deaths: Many of these deaths are avoidable through better management of blood pressure and cholesterol, and increased access to vaccination and smoking cessation programs.
The Pathophysiology of the Rural Health Gap
The increased mortality in rural populations is not merely a result of distance, but of comorbidity—the simultaneous presence of two or more chronic diseases in one patient. In rural cohorts, we spot a higher clustering of obesity, Type 2 diabetes, and hypertension. These conditions act synergistically to accelerate atherosclerosis (the buildup of fats and cholesterol in artery walls), which directly increases the incidence of ischemic strokes and myocardial infarctions.
the mechanism of action for many rural deaths involves a delay in acute care. For instance, in the case of an opioid overdose—a leading component of “unintentional injuries”—the administration of Naloxone (an opioid antagonist that displaces opioids from the mu-opioid receptors in the brain to reverse respiratory depression) is often delayed. In an urban setting, EMS arrival may occur within minutes; in rural areas, the time to administration can exceed the window of viability.

“The disparity in rural health is not a reflection of the resilience of the people, but a reflection of the fragility of the infrastructure. We are seeing a systemic failure to provide the basic continuum of care from primary prevention to acute intervention.”
This observation is echoed by epidemiologists who note that the lack of specialized care, such as neurologists for stroke or oncologists for cancer, forces rural patients to travel long distances. This often leads to “treatment fatigue” or the total abandonment of follow-up care, which is essential for managing chronic lower respiratory diseases like COPD (Chronic Obstructive Pulmonary Disease).
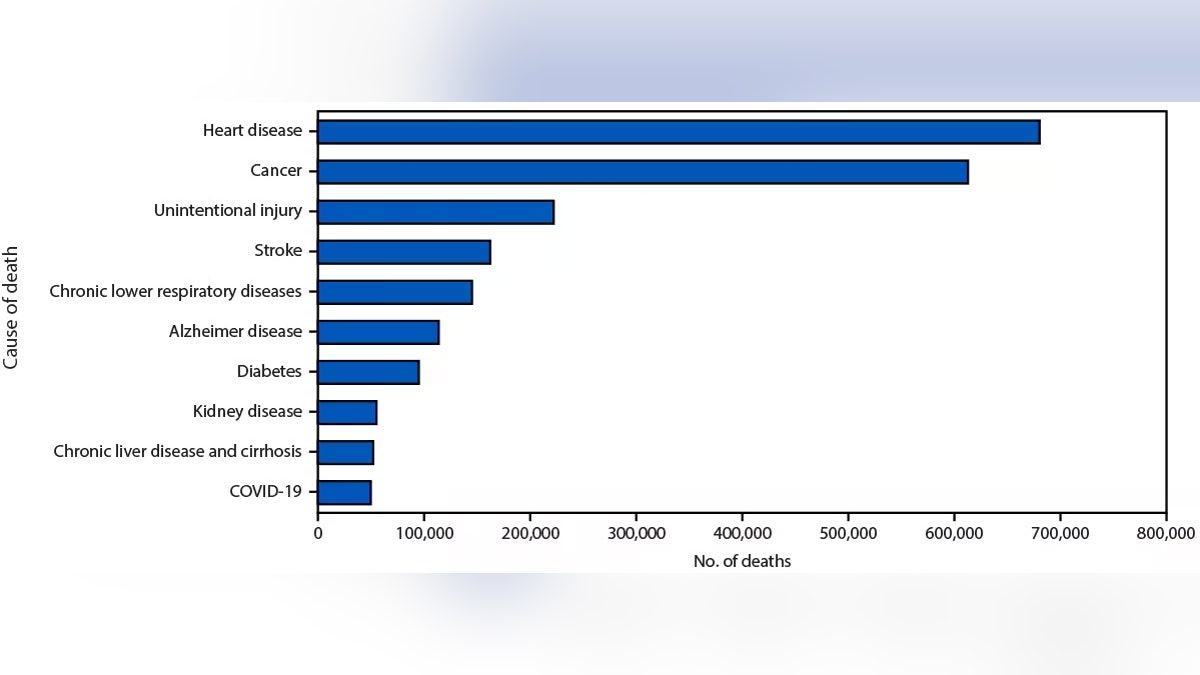
Comparative Mortality Analysis: Rural vs. Urban
The following data summarizes the increased risk profile associated with rural residency across the five leading causes of death, reflecting the trends identified in the recent CDC analysis.
| Leading Cause of Death | Rural Risk Profile | Primary Driver | Clinical Impact |
|---|---|---|---|
| Heart Disease | Higher | Hypertension/Obesity | Delayed Reperfusion Therapy |
| Cancer | Higher | Late-stage Diagnosis | Reduced Screening Adherence |
| Unintentional Injury | Significantly Higher | Opioid Crisis/Farm Accidents | Delayed Emergency Response |
| Chronic Respiratory Disease | Higher | Tobacco Use/Pollutants | Lack of Pulmonary Specialists |
| Stroke | Higher | Unmanaged Vascular Risk | Limited Access to Thrombolytics |
Geo-Epidemiological Bridging and Regulatory Hurdles
While the CDC tracks these trends in the US, the phenomenon of the “rural penalty” is global. In the United Kingdom, the NHS struggles with similar “cold spots” in healthcare delivery, though the single-payer system mitigates some financial barriers that exist in the US. In the US, the FDA has attempted to address this through the expansion of telehealth frameworks, allowing for remote monitoring of chronic conditions.
However, telehealth is only a partial solution. It cannot perform a surgical resection of a tumor or administer a catheterization for a blocked artery. The funding for the underlying research in these CDC studies is provided by federal tax dollars via the Department of Health and Human Services (HHS), ensuring that the data is free from pharmaceutical industry bias. Yet, the translation of this data into policy—such as increasing the number of federally qualified health centers (FQHCs)—remains slow.
The lack of “double-blind placebo-controlled” trials for rural-specific health interventions is a significant gap. Most medical guidelines are developed based on urban patient populations, which may not account for the specific environmental and occupational stressors found in rural farming or mining communities.
Contraindications & When to Consult a Doctor
While general health guidelines apply to all, rural patients must be hyper-vigilant about “red flag” symptoms due to the increased transit time to care. Consider seek immediate emergency medical intervention if you experience:
- Neurological Deficits: Sudden facial drooping, arm weakness, or speech difficulty (the FAST criteria for stroke).
- Cardiac Distress: Pressure, squeezing, or fullness in the center of the chest, often radiating to the left arm or jaw.
- Respiratory Failure: Sudden, severe shortness of breath or a bluish tint to the lips (cyanosis).
Note: Patients on blood thinners (anticoagulants) should be aware that rural trauma carries a higher risk of internal hemorrhage due to the delay in receiving reversal agents at a trauma center.
The Path Forward: Precision Public Health
Addressing the rural mortality gap requires a shift toward “Precision Public Health.” This involves utilizing geospatial mapping to identify “healthcare deserts” and deploying mobile screening units to conduct mammograms and colonoscopies in situ. By bringing the screening to the patient, we can move the diagnosis from Stage IV to Stage I, where the probability of survival is exponentially higher.
The trajectory of rural health depends on our ability to integrate technology with physical infrastructure. Until the shortage of primary care physicians in rural America is solved, the statistical probability of death from these five leading causes will remain stubbornly higher than in our cities. We must move beyond documenting the disparity and begin aggressively funding the deployment of specialists to the fringes of our healthcare system.