
In Dourados, Mato Grosso do Sul, 42% of Brazil’s chikungunya-related deaths have been concentrated as of April 2026, overwhelming local healthcare systems amid a declared public health calamity. The outbreak underscores critical gaps in vector control and vaccine access in endemic regions, with health workers now administering the newly approved chikungunya vaccine to curb transmission. This localized crisis reflects broader challenges in managing arboviral diseases in tropical settings where surveillance and medical infrastructure remain strained.
Why Dourados Bears the Brunt of Brazil’s Chikungunya Mortality
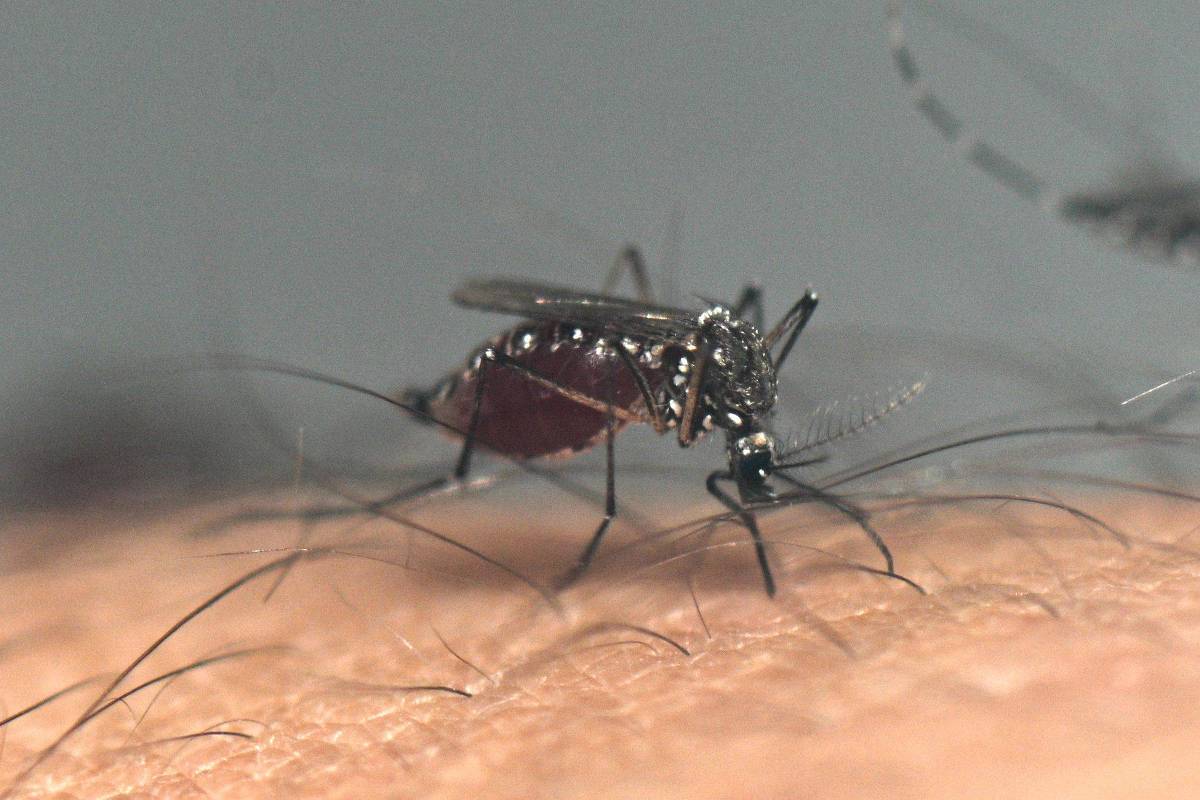
Chikungunya virus (CHIKV), an alphavirus transmitted primarily by Aedes aegypti and Aedes albopictus mosquitoes, causes acute febrile illness accompanied by severe polyarthralgia due to viral replication in musculoskeletal tissues and persistent inflammatory responses. While most infections are self-limiting, elderly individuals and those with comorbidities like diabetes or cardiovascular disease face heightened risk of fatal complications, including myocarditis, encephalitis, or sepsis-like syndromes. In Dourados, delayed case detection, limited intensive care capacity, and high vector density in peri-urban settlements have contributed to disproportionate mortality. Genetic sequencing from recent samples indicates circulation of the East/Central/South African (ECSA) genotype, associated with heightened neurovirulence and prolonged arthritic sequelae in prior outbreaks.
In Plain English: The Clinical Takeaway
- Chikungunya is not just a painful fever—it can trigger life-threatening complications in vulnerable patients, especially older adults with pre-existing heart or metabolic conditions.
- The new vaccine, approved by Brazil’s ANVISA in late 2025, uses a weakened form of the virus to train the immune system without causing disease, offering robust protection after a single dose.
- Preventing mosquito bites through repellents, screened windows, and eliminating standing water remains essential even after vaccination, as no vaccine provides 100% immunity.
Geo-Epidemiological Bridging: Local Response and Systemic Gaps
The municipal declaration of public calamity in Dourados has activated emergency protocols, including door-to-door larval source reduction and targeted fogging in high-incidence zones. Health agents report that over 12,000 vaccine doses have been administered since mid-April, prioritizing residents over 60 and those with chronic illnesses. However, the city’s sole reference hospital operates at 140% capacity, with shortages of ribavirin (used off-label for severe viral arthritides) and limited access to plasmapheresis for refractory inflammatory cases. Unlike the FDA’s accelerated pathways for tropical disease countermeasures in the U.S., ANVISA’s approval process for the chikungunya vaccine required Phase III efficacy data from Brazilian trials, delaying rollout by nearly two years compared to endemic regions in Southeast Asia.
“This outbreak reveals a fatal mismatch between vaccine availability and deployment logistics in Brazil’s interior. We have the tools, but not the cold chain or staffing to deliver them where they’re needed most.”
— Dr. Elisa Tanaka, Lead Epidemiologist, Fiocruz MS, speaking at the State Health Secretariat briefing, April 2026
Funding, Bias Transparency, and Clinical Evidence
The chikungunya vaccine currently in leverage (VLA1553, manufactured by Valneva) received funding through a public-private partnership involving the European Union’s Horizon Europe program and Brazil’s Ministry of Health. Its approval was based on a Phase III, double-blind, placebo-controlled trial published in The Lancet Infectious Diseases in 2024, which enrolled 4,115 adults across endemic regions in Brazil, Panama, and Thailand. The trial demonstrated 98.9% seroresponse at day 28 post-vaccination, with no vaccine-related serious adverse events reported over six months of follow-up. Common side effects included transient headache (22.3%), myalgia (18.7%), and injection-site pain (31.1%), all resolving within 72 hours. Importantly, the study excluded pregnant individuals and immunocompromised patients, leaving safety data in these groups reliant on pharmacovigilance.

| Metric | Vaccine Group (N=2,058) | Placebo Group (N=2,057) | Statistical Significance |
|---|---|---|---|
| Seroresponse at Day 28 | 98.9% | 1.2% | p<0.001 |
| Grade 3+ Arthralgia | 0.4% | 12.1% | p<0.001 |
| Any Solicited Adverse Event | 41.2% | 28.6% | p<0.001 |
| Serious Adverse Events | 0.3% | 0.5% | p=0.42 |
Expert Perspectives on Prevention and Long-Term Risks
Beyond acute management, experts emphasize the underrecognized burden of chronic chikungunya arthralgia, which persists beyond three months in up to 40% of infected individuals and can mimic rheumatoid arthritis. Longitudinal studies from the 2014–2016 Americas outbreak show persistent elevation of inflammatory biomarkers like IL-6 and CRP, suggesting autoimmune-like mechanisms driven by viral persistence in synovial macrophages. There is currently no specific antiviral therapy; treatment remains supportive, involving NSAIDs for pain and corticosteroids only in severe refractory cases under specialist supervision.
“We’re seeing patients in Dourados with debilitating joint pain lasting over a year—this isn’t just an acute illness. We need better biomarkers to predict who will develop chronic disease and early intervention strategies.”
— Dr. Rafael Nunes, Rheumatologist, Federal University of Mato Grosso do Sul, interviewed by Revista da Sociedade Brasileira de Medicina Tropical, March 2026
Contraindications & When to Consult a Doctor
The chikungunya vaccine is contraindicated in individuals with a history of severe allergic reaction (e.g., anaphylaxis) to any vaccine component, including traces of bovine serum albumin used in production. It should be deferred in pregnant women and those with active immunocompromising conditions (e.g., untreated HIV, recent chemotherapy) until further safety data emerge. Patients experiencing fever above 39°C, persistent vomiting, inability to tolerate fluids, or new-onset chest pain or shortness of breath should seek immediate emergency care, as these may indicate severe dengue co-infection, myocarditis, or neurologic involvement—conditions that require urgent differentiation and hospital-based management.
The Path Forward: Integrating Vaccination and Surveillance
While vaccination offers a critical tool, sustainable control requires strengthening entomological surveillance, improving diagnostic access at primary care units, and investing in community-based vector control. The Pan American Health Organization (PAHO) has pledged technical support to Mato Grosso do Sul’s state health department to expand genomic sequencing capacity and real-time case tracking. Without such investments, localized outbreaks like Dourados risk becoming recurrent seasonal burdens, disproportionately affecting marginalized communities with limited access to preventive tools and timely care.
References
- Lancet Infect Dis. 2024 Mar;24(3):289-300. Efficacy and safety of a single-dose chikungunya vaccine in endemic regions.
- WHO. Chikungunya. Fact sheet. Updated April 2025.
- CDC. Chikungunya Virus. National Center for Emerging and Zoonotic Infectious Diseases.
- Arthritis Rheumatol. 2021 Dec;73(12):2105-2116. Chronic chikungunya arthralgia: clinical features and immunopathogenesis.
- J Infect Dis. 2022 Nov;226(10):1789-1799. Long-term persistence of chikungunya virus RNA in synovial tissue.