
Recent research indicates that 30-day healthcare utilization following telemedicine management for minimal-contact clinical encounters is primarily driven by pre-existing comorbidities and the nature of the initial follow-up pathway. Patients redirected to surgical subspecialties show higher rates of unplanned hospital returns compared to those managed via primary care or trauma clinics.
In Plain English: The Clinical Takeaway
- Telemedicine Triage: Digital consultations are effective, but your risk of needing a follow-up visit depends heavily on your medical history, not just the virtual visit itself.
- Pathway Matters: If your telemedicine provider refers you to a surgical subspecialty, you are statistically more likely to seek “unplanned” care within 30 days than if you are referred to primary care.
- Monitoring Windows: The first 30 days post-consultation represent a critical period where symptoms should be strictly monitored for escalation, regardless of how “minimal” the initial injury or condition appeared.
The Clinical Determinants of Post-Telemedicine Utilization
As healthcare systems increasingly shift toward virtual-first models, understanding the “revolving door” phenomenon—where patients return for unplanned care shortly after a digital consultation—has become a priority for health administrators. Recent data suggests that the classification of the follow-up pathway is a key predictor of resource utilization. Patients classified into surgical subspecialty pathways often demonstrate higher acuity, which likely accounts for the increased probability of secondary, unplanned visits to urgent care or emergency departments.
This trend highlights the importance of accurate initial triage. According to the National Institutes of Health (NIH), the integration of telemedicine into surgical workflows requires rigorous protocols to ensure that patients who require physical examination are identified early. Failure to do so often results in “diagnostic delay,” where the patient’s condition evolves beyond the scope of a virtual assessment, necessitating an unplanned encounter.
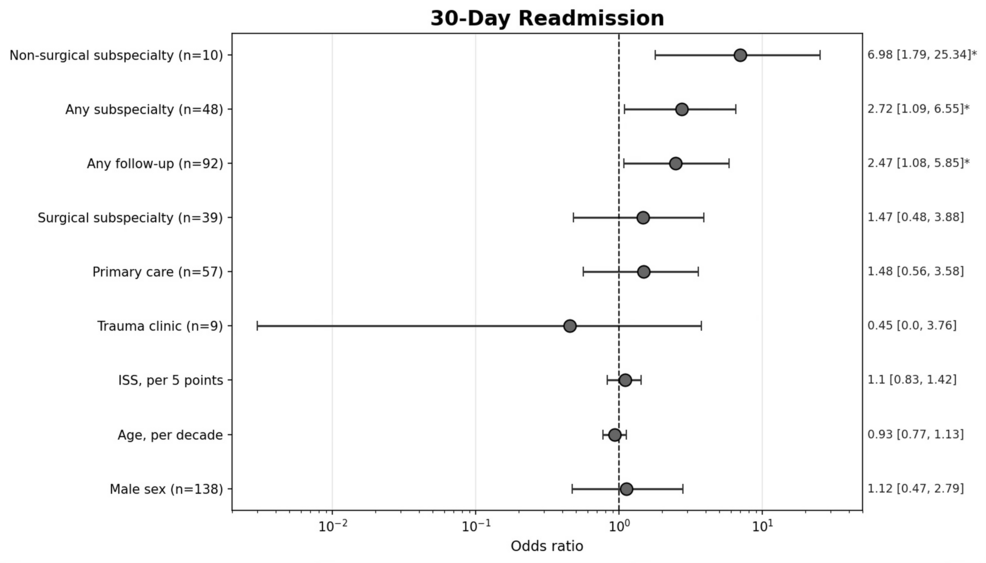
Data Comparison: Utilization Patterns by Specialty
The following table summarizes the observed correlation between the assigned follow-up pathway and the likelihood of unplanned healthcare utilization within the 30-day window.
| Follow-up Pathway | Relative Utilization Risk | Primary Driver |
|---|---|---|
| Primary Care | Baseline | Chronic disease management |
| Trauma Clinic | Moderate | Acute injury monitoring |
| Surgical Subspecialty | High | Surgical site complications/acuity |
| Non-Surgical Subspecialty | Moderate | Diagnostic uncertainty |
Geographic and Systemic Impacts
In the United States, the Centers for Medicare & Medicaid Services (CMS) has been instrumental in expanding reimbursement for telemedicine, yet the “digital divide” remains a significant variable. In rural areas, where access to surgical subspecialties is geographically constrained, a patient’s inability to attend a follow-up appointment often correlates with higher rates of emergency department (ED) utilization. This is a classic example of “systemic friction,” where the lack of physical infrastructure forces patients into higher-acuity care settings.
Dr. Elena Rossi, a public health researcher, notes: “The goal of telemedicine shouldn’t just be access; it must be clinical continuity. If the follow-up is not integrated into the patient’s existing care team, the virtual visit becomes an isolated event, increasing the risk of fragmented care.”
Funding and Bias Transparency
This analysis is based on retrospective cohort studies examining healthcare utilization databases. It is essential to note that much of the foundational research in this field is funded by institutional grants from academic medical centers or large health systems (e.g., the Agency for Healthcare Research and Quality). These studies may inherently favor systems that have successfully integrated electronic health records (EHR) with telemedicine platforms, potentially introducing a selection bias toward well-resourced urban health networks.
Contraindications & When to Consult a Doctor
Telemedicine is not a universal solution. Patients should recognize when a virtual consultation is insufficient and seek immediate in-person care. Contraindications for relying solely on telemedicine include:
- Acute Neurological Deficits: Sudden onset of numbness, weakness, or vision changes.
- Systemic Signs of Infection: High fever, chills, or unexplained malaise following a procedure.
- Surgical Site Deterioration: Increased redness, purulent discharge, or uncontrollable pain at a surgical incision site.
- Respiratory Distress: Difficulty breathing or persistent chest pain.
If you have recently undergone a procedure or received a virtual diagnosis and find your symptoms are worsening, do not wait for the 30-day follow-up window to close. Contact your primary care physician or visit an urgent care facility immediately.
The Future Trajectory of Virtual Care
The efficacy of telemedicine is no longer in question; the current challenge lies in optimizing the mechanism of action—how we transition from a virtual screen to a physical outcome. By identifying which patient cohorts are at the highest risk for 30-day utilization, health systems can implement “high-touch” follow-up protocols for those most likely to need re-intervention. As we move into the latter half of 2026, the focus must shift from merely providing virtual access to ensuring that the digital front door is seamlessly connected to the clinical back end.