
The Crohn’s Disease Exclusion Diet (CDED), when combined with partial enteral nutrition, serves as an effective alternative to exclusive enteral nutrition (EEN) for inducing remission in pediatric Crohn’s disease. Research published in Nature indicates that both dietary protocols achieve similar clinical outcomes, providing patients with more flexible, sustainable treatment options.
In Plain English: The Clinical Takeaway
- Dietary Flexibility: Unlike Exclusive Enteral Nutrition (EEN), which requires patients to consume only liquid formula for weeks, the Crohn’s Disease Exclusion Diet (CDED) allows for specific whole foods, improving patient adherence.
- Equivalency in Remission: Clinical data confirms that CDED is non-inferior to EEN, meaning it is just as effective at reducing inflammation in the digestive tract.
- Maintenance of Microbiome: Emerging evidence suggests that whole-food diets may better support long-term gut health compared to highly processed liquid-only formulas.
The Shift from Liquid Formulas to Whole-Food Protocols
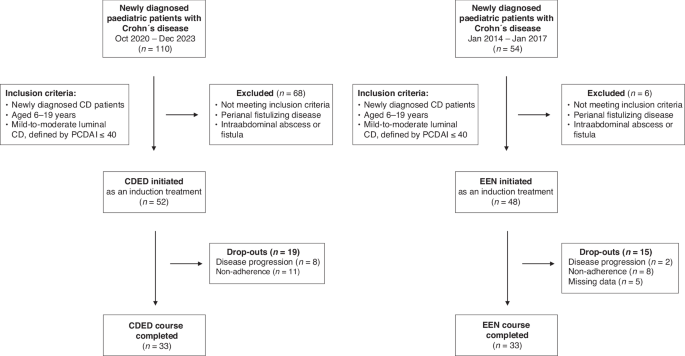
For decades, Exclusive Enteral Nutrition (EEN) has been the gold standard for inducing remission in pediatric Crohn’s disease. EEN involves a strict regimen where the patient consumes only a liquid, nutritionally complete formula for six to eight weeks. While effective, the high rate of non-adherence due to the restrictive nature of the diet has prompted researchers to seek alternatives. The Crohn’s Disease Exclusion Diet (CDED) was developed to address this limitation by pairing partial enteral nutrition—where formula provides roughly 50% of caloric intake—with a structured, whole-food diet designed to minimize exposure to food components that may trigger inflammation, such as certain emulsifiers and saturated fats.
Recent clinical analysis published in Nature confirms that this hybrid approach does not compromise efficacy. By focusing on the exclusion of specific dietary triggers while maintaining nutritional adequacy through formula, clinicians are seeing pediatric patients reach clinical remission at rates comparable to those undergoing traditional EEN. This development is significant for gastrointestinal health, as it reduces the social and psychological burden often associated with liquid-only diets in school-aged children.
Clinical Efficacy and Comparative Data
The mechanism of action for both EEN and CDED centers on modulating the gut microbiome and reducing intestinal inflammation. EEN acts by providing easily absorbable nutrients while resting the bowel, whereas CDED works by systematically eliminating dietary antigens that may disturb the intestinal barrier. According to research findings, the induction of remission is statistically similar between the two groups, though adherence rates are significantly higher in the CDED cohort.
| Treatment Protocol | Primary Mechanism | Adherence Potential | Clinical Outcome |
|---|---|---|---|
| Exclusive Enteral Nutrition (EEN) | Bowel rest; liquid-only formula | Low (Restrictive) | High Remission Rate |
| Crohn’s Disease Exclusion Diet (CDED) | Antigen exclusion; partial liquid support | Moderate to High | Non-inferior to EEN |
Funding, Transparency, and Global Accessibility
The underlying research into CDED has been supported by various institutional grants aimed at improving pediatric inflammatory bowel disease (IBD) care. It is important for patients and caregivers to note that while these diets are evidence-based, they require strict medical supervision. In the United States, the FDA regulates clinical nutrition products, but dietary interventions remain largely under the purview of specialized pediatric gastroenterologists and registered dietitians.
Dr. Arie Levine, a lead researcher in the field of pediatric IBD, has long advocated for the shift toward structured food-based therapies. In peer-reviewed discussions, he has emphasized that `The goal of modern IBD management is to achieve mucosal healing while maintaining a quality of life that allows children to participate in normal social and dietary activities.` This sentiment aligns with current shifts in guidelines from organizations such as the European Crohn’s and Colitis Organisation (ECCO).
Contraindications & When to Consult a Doctor
Neither EEN nor CDED should be initiated without the guidance of a pediatric gastroenterologist. Patients with severe stricturing Crohn’s disease—where the bowel is narrowed and at risk of obstruction—must be monitored closely, as solid food introduction in these cases requires specific medical clearance. Furthermore, these diets are not a substitute for pharmacological interventions, such as biologics or immunomodulators, in patients who require systemic immune suppression to manage disease progression. If a child experiences persistent abdominal pain, unexplained weight loss, or bloody stools, immediate consultation with a specialist is required to prevent permanent intestinal damage.
Future Trajectory in Pediatric Gastroenterology
The success of the CDED protocol suggests a move toward personalized nutritional therapy in the management of autoimmune conditions. As longitudinal data matures, researchers are looking at how these dietary shifts affect long-term maintenance of remission without the constant need for aggressive medication. While EEN remains a viable tool, the evidence-based move toward CDED provides families with a more sustainable roadmap for managing Crohn’s disease in the long term.
References
- Levine, A., et al. (2019). Crohn’s disease exclusion diet plus partial enteral nutrition versus exclusive enteral nutrition for induction of remission in children with Crohn’s disease. Gastroenterology.
- The Lancet Gastroenterology & Hepatology: Nutritional therapy in IBD.
- Nature Reviews Gastroenterology & Hepatology: Dietary management of Crohn’s disease.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.