
The U.S. is currently managing a rise in Cyclospora cayetanensis infections, a parasitic illness causing severe gastrointestinal distress. Transmitted via contaminated fresh produce, these outbreaks require rapid public health intervention. Standard diagnostic testing is essential, as the parasite remains resilient, necessitating precise antibiotic protocols to mitigate widespread community transmission risks.
In Plain English: The Clinical Takeaway
- The Cause: Cyclosporiasis is an intestinal infection caused by a microscopic parasite. It is not contagious person-to-person; it is contracted by consuming food or water contaminated with infected fecal matter.
- The Symptoms: Watch for “explosive” watery diarrhea, loss of appetite, weight loss, and intense fatigue. Symptoms often appear about one week after exposure.
- The Treatment: Unlike bacterial infections, this requires specific anti-parasitic medication. If you suspect infection, see a physician for a stool ova and parasite (O&P) exam, as standard bacterial cultures will not detect this organism.
The Biological Mechanism of Cyclospora Infection
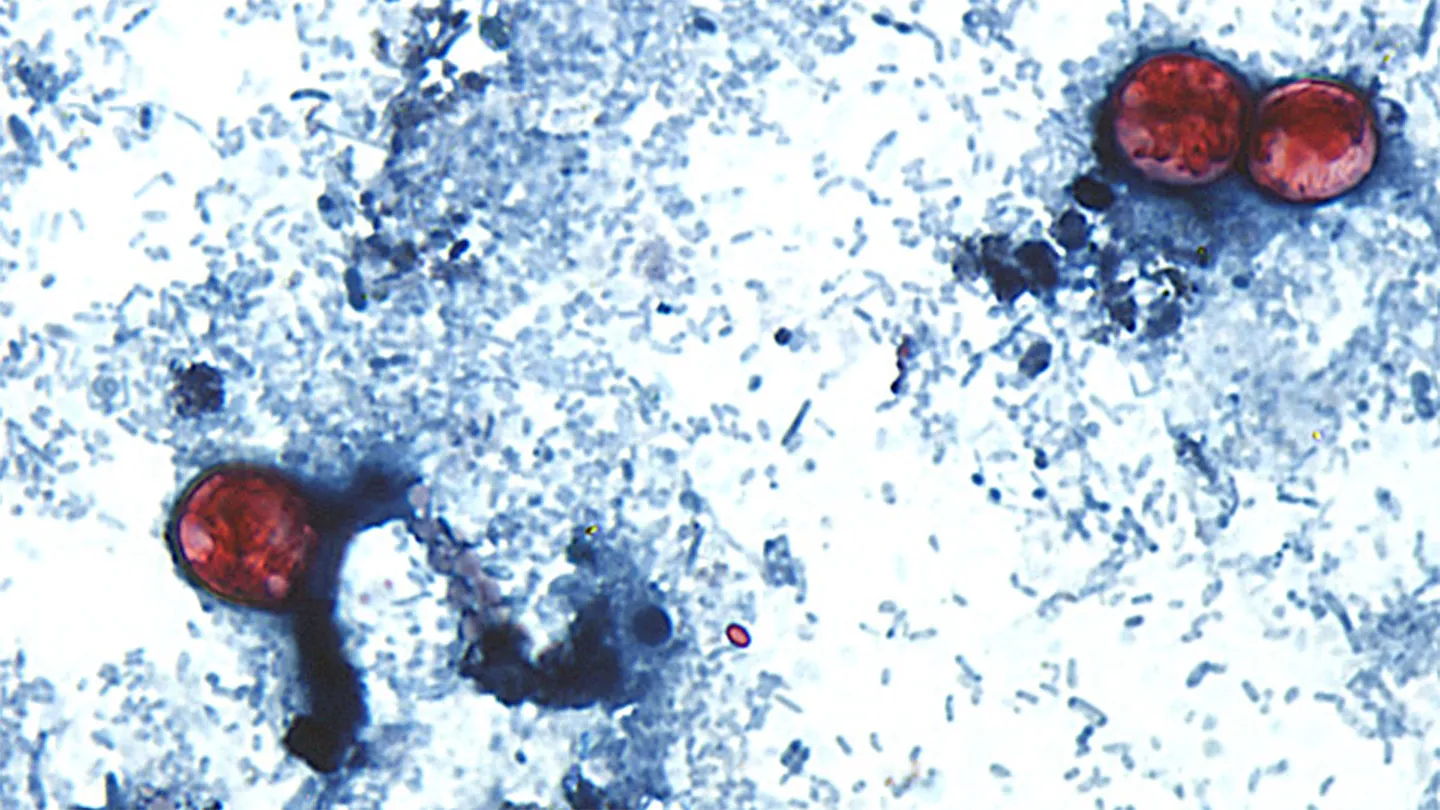
Cyclospora cayetanensis is a coccidian protozoan that primarily invades the epithelial cells of the small intestine. Once ingested—usually through contaminated cilantro, basil, or imported berries—the oocysts undergo excystation in the gastrointestinal tract. This triggers an inflammatory response in the mucosal lining, leading to malabsorption and the characteristic “explosive” diarrhea that defines the clinical presentation.
Unlike common foodborne pathogens like Salmonella or E. coli, Cyclospora is not immediately infectious upon excretion. According to the Centers for Disease Control and Prevention (CDC), the oocysts must undergo a maturation process in the environment, which can take several days to weeks. This biological delay is a critical factor in why outbreaks are often linked to produce supply chains rather than immediate point-source contamination.
Epidemiological Challenges and Regulatory Surveillance
In the United States, the Food and Drug Administration (FDA) and the CDC coordinate to trace these outbreaks back to specific agricultural regions. The primary challenge lies in the parasite’s resilience; the oocysts are hardy and can survive in water and soil for extended periods. As of mid-July 2026, health departments are utilizing molecular subtyping to link disparate cases, a process that requires time-sensitive reporting from clinical laboratories.
Dr. Maria Elena Bottazzi, a noted researcher in tropical medicine, notes: `The difficulty with Cyclospora lies in its environmental persistence. Because the parasite requires a developmental phase outside the host, our surveillance must look beyond the immediate kitchen and toward the irrigation and harvesting practices of global produce distribution networks.`
| Feature | Cyclospora | Salmonella |
|---|---|---|
| Pathogen Type | Protozoan | Bacterium |
| Incubation Period | ~7 days | 6–72 hours |
| Standard Treatment | Trimethoprim-sulfamethoxazole | Usually supportive care |
| Testing Method | Stool O&P/PCR | Stool Culture |
Contraindications & When to Consult a Doctor
The standard pharmacologic intervention for cyclosporiasis is a combination of trimethoprim and sulfamethoxazole (TMP-SMX). However, this treatment is not universal. Patients with a known hypersensitivity to sulfonamides must consult an infectious disease specialist for alternative therapies, such as ciprofloxacin, though the latter demonstrates lower efficacy rates in clinical trials.
Seek immediate medical attention if you experience:
- Signs of severe dehydration (dizziness, dry mouth, decreased urine output).
- Fever exceeding 101.5°F (38.6°C).
- Persistent symptoms lasting longer than 48 hours despite conservative management.
- Bloody stools (which are atypical for Cyclospora and may indicate a different pathogen).
The Future of Outbreak Mitigation
The fight against Cyclospora is evolving as genomic sequencing becomes a standard tool in public health. By mapping the genetic signature of the parasite, researchers are moving closer to identifying the specific agricultural water sources responsible for contamination. While research into vaccine development remains in early, pre-clinical phases, the current focus remains on rigorous produce washing and improved supply chain transparency.
Funding for ongoing epidemiological research is primarily provided by the National Institutes of Health (NIH) and the FDA’s Food Safety Modernization Act (FSMA) initiatives. There are no known industry-funded conflicts of interest regarding the standard treatment protocols for this parasitic infection.
References
- National Library of Medicine: Cyclospora cayetanensis – Pathophysiology and Clinical Management
- CDC Morbidity and Mortality Weekly Report (MMWR) – Foodborne Outbreak Surveillance
- World Health Organization: Food Safety and Parasitic Infections
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the counsel of your physician or qualified health provider for any questions regarding a medical condition.