
An 11-year-old child recently presented with midgut volvulus secondary to intestinal malrotation, a rare clinical scenario where the bowel twists around its blood supply. Despite the potential for catastrophic tissue death, the patient maintained preserved bowel viability, highlighting the critical importance of early surgical intervention and diagnostic vigilance in pediatric care.
In Plain English: The Clinical Takeaway
- What is it? Intestinal malrotation is a congenital (present at birth) condition where the intestines do not settle into their normal position, making them prone to twisting, known as a volvulus.
- The Danger: This twisting can cut off blood flow to the gut, leading to rapid tissue death (necrosis).
- The Good News: When identified early—even in older children—surgical correction can save the bowel before permanent damage occurs.
The Mechanics of Midgut Volvulus and Developmental Anatomy
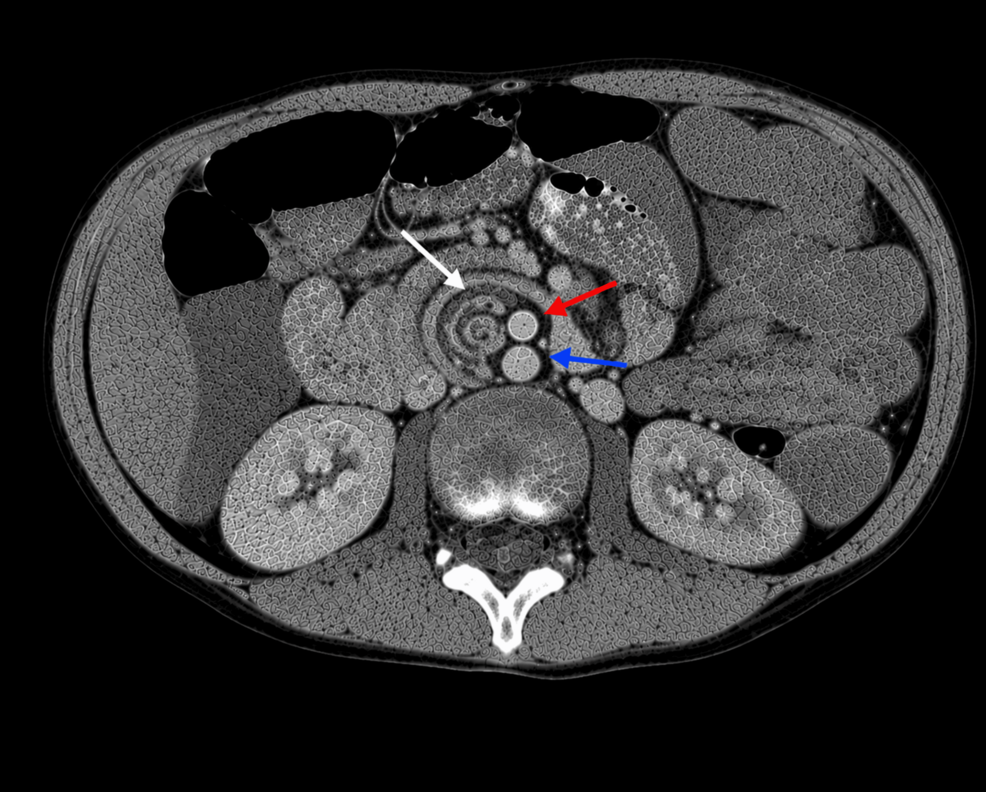
During fetal development, the midgut normally undergoes a complex rotation and fixation process within the abdominal cavity. When this process is interrupted, the mesenteric base—the tissue attaching the intestines to the abdominal wall—remains narrow. This anatomical anomaly creates a “pedicle” or stalk that acts as a pivot point for the small intestine to rotate around the superior mesenteric artery.
The mechanism of action in a volvulus is essentially mechanical obstruction combined with vascular compromise. As the bowel twists, it creates a closed-loop obstruction. If the twist is not reduced immediately, venous congestion occurs, followed by arterial occlusion, eventually leading to ischemic necrosis—the death of tissue due to lack of oxygen. In the case of the 11-year-old patient, the delayed presentation is particularly noteworthy because such cases are traditionally associated with infants under the age of one. According to clinical data published in Cureus, the rarity of this presentation in older children often leads to diagnostic delays, as clinicians may not prioritize malrotation in the differential diagnosis for abdominal pain in pre-adolescents.
Diagnostic Challenges and Epidemiological Context
Diagnosing malrotation in older children requires a high index of suspicion. Symptoms are often intermittent and non-specific, ranging from chronic abdominal pain and bilious vomiting to failure to thrive. Unlike the acute, dramatic presentation seen in neonates, older children often experience “subacute” or chronic symptoms, which can mask the underlying surgical emergency.
Epidemiologically, intestinal malrotation is estimated to occur in 1 in 500 to 1 in 6,000 live births. However, many cases remain asymptomatic throughout life. The shift in presentation toward older pediatric populations suggests that the “twist” may be incomplete or intermittent, allowing for spontaneous detorsion before infarction occurs. This specific case underscores the necessity of utilizing advanced imaging, such as an upper gastrointestinal (GI) contrast study, which remains the gold standard for identifying the position of the duodenojejunal junction.
| Clinical Feature | Infant Presentation | Older Child Presentation |
|---|---|---|
| Primary Symptom | Bilious vomiting (acute) | Recurrent abdominal pain |
| Diagnostic Speed | Rapid (hours) | Delayed (weeks/months) |
| Bowel Viability Risk | Extremely High | Variable (depending on chronicity) |
Bridging the Gap: Healthcare Systems and Access
The management of intestinal malrotation is standardized globally through the Ladd’s procedure, a surgical intervention that involves untwisting the bowel, dividing fibrous bands (Ladd’s bands), and broadening the mesenteric base. In the United Kingdom, the NHS emphasizes the role of pediatric surgical centers in identifying these anomalies early to prevent short bowel syndrome, a condition where the body cannot absorb enough nutrients due to loss of surface area.
In the United States, the FDA monitors the technological advancements in minimally invasive surgical tools that facilitate these procedures. However, the primary barrier to better outcomes is not technological but diagnostic. As Dr. Samuel Alaish, a pediatric surgeon, has noted in broader surgical literature, “The challenge is that the symptoms are often dismissed as simple functional abdominal pain, delaying the life-saving imaging that would reveal the rotated anatomy.”
Contraindications & When to Consult a Doctor
There are no “treatments” for malrotation other than surgical correction; however, the primary contraindication to waiting is the presence of systemic signs of sepsis or shock. If a child presents with the following, immediate emergency medical attention is required:
- Bilious (green or yellow-green) vomiting: This is a red-flag symptom indicating a possible obstruction.
- Abdominal distension and tenderness: Signs of a compromised gut.
- Signs of shock: Tachycardia (rapid heart rate), lethargy, or cool, clammy skin.
Parents should never attempt to manage recurrent, severe abdominal pain with over-the-counter analgesics alone. If your child has a history of intermittent abdominal pain that does not resolve with standard dietary adjustments, request a referral to a pediatric gastroenterologist for an evaluation of anatomical abnormalities.
The Future of Pediatric Surgical Surveillance
While the case of this 11-year-old was successful, the underlying research highlights a significant need for increased awareness among primary care physicians. As we move further into 2026, the integration of point-of-care ultrasound in emergency departments may provide a faster, radiation-free path to diagnosis, potentially reducing the time between symptom onset and surgical intervention. The focus remains on maintaining high clinical suspicion even when the patient does not fit the “classic” age profile for a congenital defect.
References
- Puntis, J. W. (2018). “Intestinal malrotation.” Paediatrics and Child Health.
- Dunn, S. P. (2023). “Malrotation.” StatPearls [Internet].
- The Lancet Child & Adolescent Health (2020). “Pediatric surgical emergencies: A global perspective.”
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.