
Researchers from the Children’s Hospital of Philadelphia (CHOP) have identified that over 25% of pediatric malaria cases in the U.S. Face significant diagnostic delays. These delays increase the risk of severe complications, highlighting a critical gap in clinician awareness for travel-related febrile illnesses in non-endemic regions.
The implications of these findings are profound. In a non-endemic environment—where malaria is not naturally occurring—physicians often suffer from a cognitive bias, overlooking the possibility of a parasitic infection in favor of more common local viruses. For a child, this gap between the onset of fever and the administration of the correct antimalarial medication can be the difference between a routine recovery and life-threatening organ failure.
In Plain English: The Clinical Takeaway
- Travel History is Key: If a child develops a fever after visiting a region where malaria is common, doctors must test for it immediately, even if other symptoms seem like a common cold.
- Time is Tissue: Delays in diagnosis allow the parasite to multiply rapidly in the blood, which can lead to severe complications like anemia or brain swelling.
- Prevention is Not a Guarantee: Even if a child took preventative medication (prophylaxis), they can still contract malaria; the medication reduces risk but does not eliminate it.
The Pathophysiology of Diagnostic Failure in Non-Endemic Zones
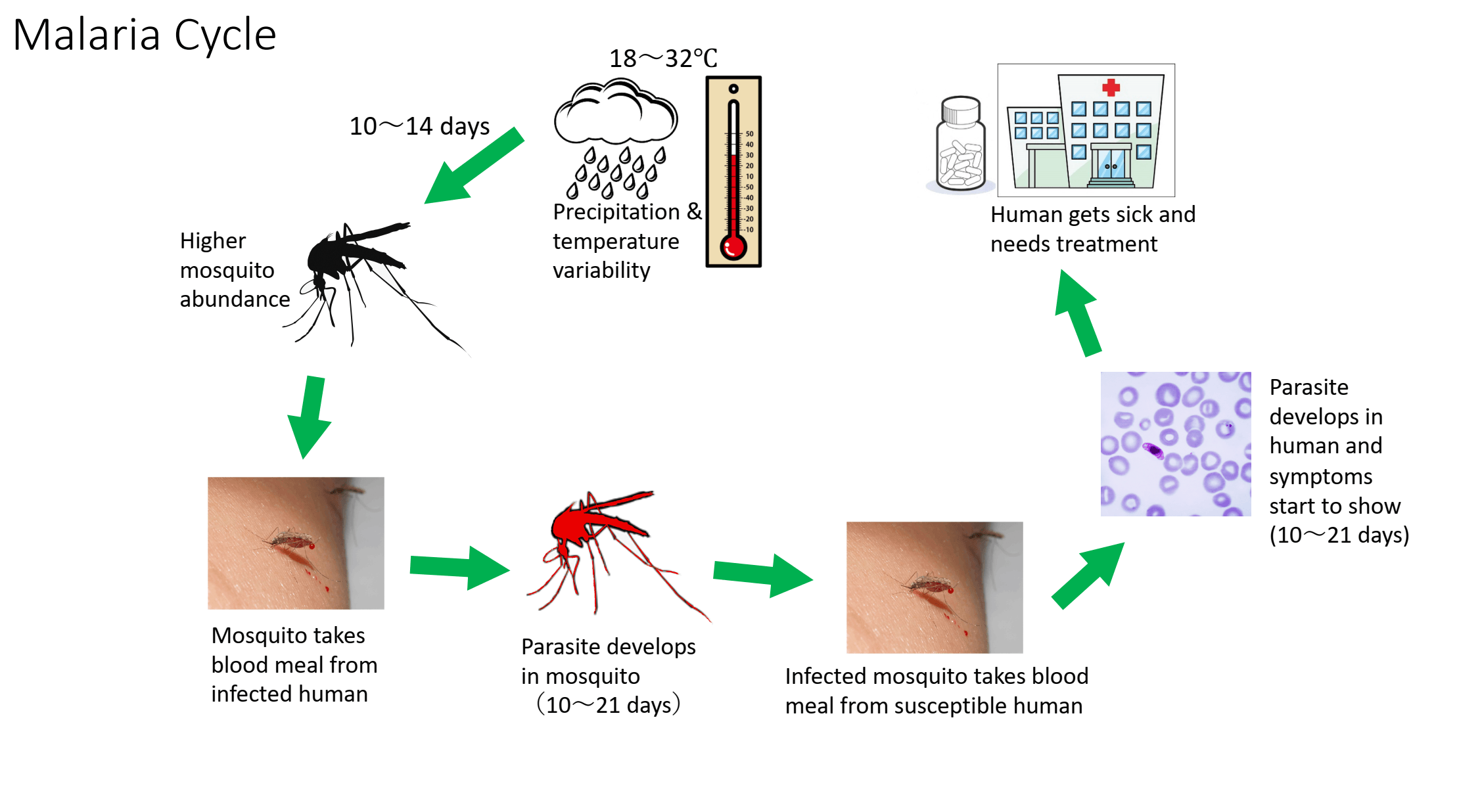
The primary challenge lies in the mechanism of action—the specific biological process—of the Plasmodium parasite. Once an infected mosquito bites a human, the parasites travel to the liver and then invade red blood cells. This erythrocytic cycle causes the cells to rupture, releasing toxins that trigger a systemic inflammatory response, resulting in the characteristic cyclical fevers of malaria.
In the United States, most pediatric cases are “imported,” meaning the infection was acquired abroad. Because U.S. Clinicians rarely encounter malaria, the “index of suspicion” remains low. This often leads to a diagnostic odyssey where patients are treated for influenza or bacterial pneumonia before a blood smear is finally ordered. When the delay extends beyond a few days, the risk of Plasmodium falciparum causing cerebral malaria—where infected cells clog the compact blood vessels in the brain—increases exponentially.
“The diagnostic gap in the U.S. Is not a failure of technology, but a failure of clinical suspicion. We have the gold-standard tools available, but they are only utilized when the clinician connects the dots between travel history and febrile symptoms,” says a senior epidemiologist specializing in tropical medicine.
Comparing Parasitic Strains and Clinical Urgency
Not all malaria is created equal. The severity of the diagnostic delay depends heavily on the species of the parasite. P. Falciparum is the most lethal and requires immediate intervention to prevent death. In contrast, P. Vivax can remain dormant in the liver as “hypnozoites,” causing relapses months after the child has returned home, further confusing the diagnostic picture.

| Parasite Species | Primary Risk Factor | Incubation Period | Clinical Hallmark |
|---|---|---|---|
| P. Falciparum | High risk of severe/cerebral malaria | 7–30 days | Rapid progression, high parasite load |
| P. Vivax | Relapsing infections (hypnozoites) | 12 days to several months | Intermittent fever, milder initial onset |
| P. Ovale/malariae | Chronic, low-grade infection | Variable (can be years) | Slow progression, renal complications |
Geo-Epidemiological Bridging: The Role of Global Health Systems
This issue is not unique to the U.S., but the systemic response varies. While the CDC provides rigorous “Yellow Book” guidelines for travelers, the translation of these guidelines into the emergency room remains inconsistent. In contrast, the UK’s NHS often utilizes more centralized travel clinics that flag returning patients for specific screenings, potentially reducing the delay seen in the more fragmented U.S. Healthcare system.
The funding for the CHOP study, largely supported by institutional grants and federal health research initiatives, underscores the need for a standardized “Travel Fever Protocol” in U.S. Pediatric emergency departments. Without a mandated screening for all pediatric febrile patients with a history of travel to endemic zones, the 25% delay rate is likely to persist.
Addressing the “Prophylaxis Paradox”
A significant contributor to diagnostic delay is the “prophylaxis paradox.” This occurs when a clinician assumes that because a child was prescribed preventative medication (such as Atovaquone-proguanil or Doxycycline), they cannot have malaria. This is a dangerous clinical assumption. No prophylactic regimen is 100% effective due to varying patient adherence and the emergence of drug-resistant strains of parasites.
To combat this, clinicians must employ a double-blind mindset—treating the patient’s symptoms as the primary evidence rather than relying on the presumed efficacy of a preventative drug. The gold standard for diagnosis remains the thick and thin blood smear, which allows a pathologist to identify the parasite under a microscope and determine the “parasitemia” (the percentage of infected red blood cells).
Contraindications & When to Consult a Doctor
Malaria is a medical emergency. Parents and caregivers should seek immediate professional medical intervention if a child exhibits the following symptoms after traveling to a malaria-endemic region:
- High Fever and Chills: Especially if the fever occurs in cycles or is accompanied by intense shivering.
- Jaundice: A yellowing of the skin or eyes, indicating liver stress or severe hemolysis (breakdown of red blood cells).
- Altered Mental State: Extreme lethargy, confusion, or seizures, which may indicate cerebral malaria.
- Severe Anemia: Unusual paleness or shortness of breath.
Note: Do not attempt to treat suspected malaria with over-the-counter antipyretics alone, as this may mask the fever while the parasite continues to proliferate.
The findings from CHOP serve as a critical wake-up call for the American medical community. By shifting the clinical culture from “passive observation” to “active suspicion” for returning travelers, we can close the diagnostic gap and prevent avoidable pediatric tragedies. The goal is a healthcare system where a travel history is treated as a vital sign, not a footnote.