
Ebstein Anomaly is a rare congenital heart defect where the tricuspid valve is malformed and displaced downward into the right ventricle. This structural failure leads to severe tricuspid regurgitation and right heart failure, requiring precise multi-modal imaging and specialized surgical intervention to restore cardiac function and patient longevity.
For patients and clinicians, the stakes are high. When the tricuspid valve fails to seal, blood flows backward into the right atrium, causing the heart to enlarge and potentially triggering life-threatening arrhythmias. This isn’t just a surgical challenge; it’s a lifelong management journey that requires a coordinated effort between cardiologists, radiologists, and surgeons to prevent permanent heart failure.
In Plain English: The Clinical Takeaway
- The Core Problem: The “door” between the upper and lower right chambers of the heart is misplaced and leaky, forcing the heart to work harder to pump blood to the lungs.
- The Diagnostic Gold Standard: While EKGs provide clues, 3D Echocardiography and Cardiac MRI are the only ways to accurately map the heart’s anatomy before surgery.
- The Treatment Goal: Surgery doesn’t always “fix” the valve perfectly, but it aims to stop the backward leak (regurgitation) and reduce the pressure in the heart.
The Pathophysiology of Tricuspid Displacement and Right Ventricular Atrialization
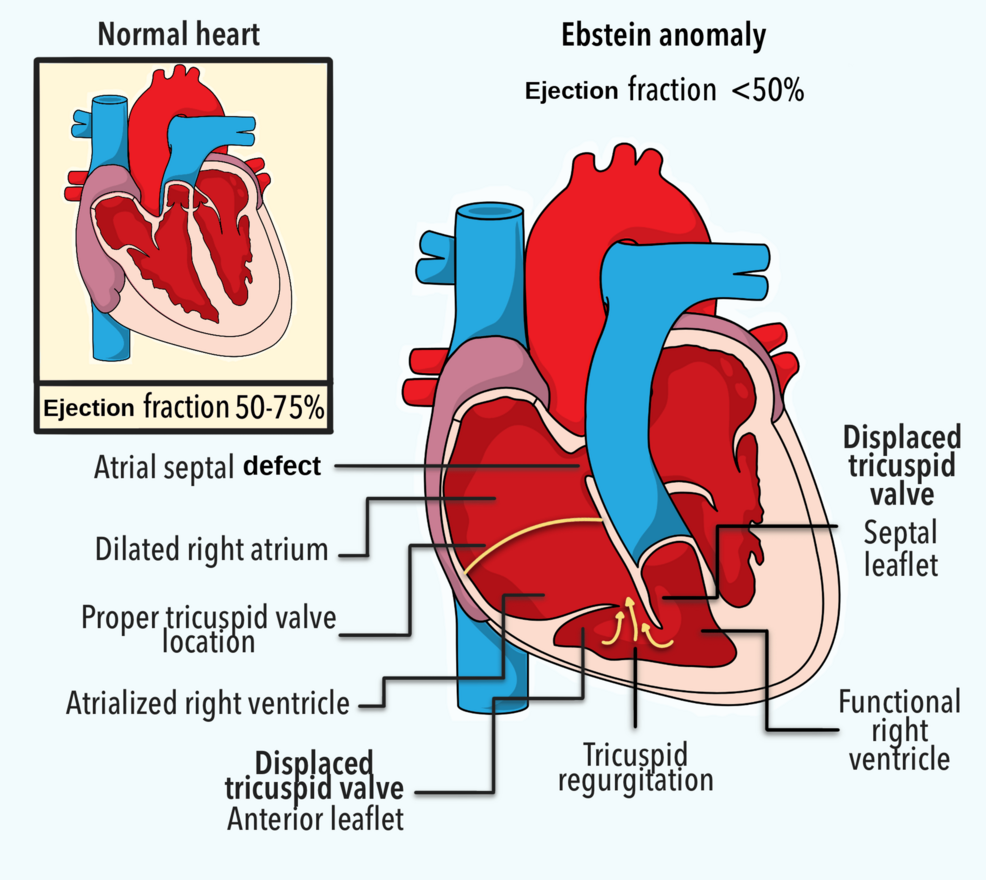
In a healthy heart, the tricuspid valve separates the right atrium from the right ventricle. In Ebstein Anomaly, the valve leaflets fail to attach properly. Instead, they are displaced toward the apex (the bottom) of the heart. This creates a phenomenon known as “atrialization” of the right ventricle.
Essentially, the upper part of the right ventricle becomes a functional extension of the right atrium. This increases the volume of the atrium and decreases the effective pumping capacity of the ventricle. The mechanism of action here is a failure of delamination during embryonic development, which prevents the valve from forming its distinct ring.
According to the PubMed database of congenital heart diseases, this structural abnormality often leads to a “right-to-left shunt” if a hole exists in the heart wall (atrial septal defect), meaning oxygen-poor blood bypasses the lungs and enters the systemic circulation, causing cyanosis—a bluish tint to the skin.
Advanced Imaging: Moving Beyond the Standard Echocardiogram
Diagnosing Ebstein Anomaly requires more than a cursory glance. While a 12-lead ECG often shows “P-mitrale” (an abnormal P-wave indicating an enlarged right atrium), imaging is where the definitive map is drawn. 3D Echocardiography allows surgeons to visualize the exact degree of leaflet displacement in real-time.
However, Cardiac MRI (CMR) provides the most rigorous data on ventricular volume and the “fractional area change.” CMR is essential for quantifying the exact amount of blood leaking backward, which dictates whether a patient needs immediate surgery or can be managed with medication. In the US, the FDA-approved use of high-resolution MRI protocols has standardized how these anomalies are graded across different healthcare systems.
| Imaging Modality | Primary Clinical Utility | Key Limitation |
|---|---|---|
| Transthoracic Echo (TTE) | Initial screening; valve morphology | Lower resolution in obese patients |
| 3D Echocardiography | Pre-surgical mapping of leaflets | Operator dependent; “noise” in images |
| Cardiac MRI (CMR) | Gold standard for volume/function | Cost; availability; contraindicated by some metal implants |
| Cardiac CT | Anatomical relationship to coronary arteries | Radiation exposure; contrast requirements |
Therapeutic Interventions: From the Cone Procedure to Medical Management
Therapeutics for Ebstein Anomaly are categorized by the severity of the regurgitation. For mild cases, pharmacological management focuses on diuretics to reduce fluid buildup in the lungs and abdomen. However, for moderate to severe cases, surgical intervention is the only viable path.
The “Cone Reconstruction” technique is currently the gold standard. This procedure involves mobilizing the valve leaflets and “coning” them together to create a functional, leak-proof valve. This reduces the size of the right atrium and restores the ventricle’s ability to pump blood forward. This approach has significantly improved long-term survival rates compared to older methods of valve replacement, which often required lifelong anticoagulation therapy.
In Europe, the European Medicines Agency (EMA) and various national health services, such as the NHS in the UK, have integrated multidisciplinary “Heart Teams” to decide the timing of these surgeries. The goal is to operate before the right ventricle becomes so dilated that it cannot recover, a state known as irreversible heart failure.
Regarding funding and bias, much of the foundational research into these surgical techniques is funded by academic medical centers and non-profit congenital heart foundations. Because there is no single “drug” to cure a structural defect, the research is primarily driven by surgical outcomes and longitudinal patient registries rather than pharmaceutical profit.
Contraindications & When to Consult a Doctor
Surgical intervention is not a universal solution. Contraindications for aggressive surgical reconstruction include severe pulmonary hypertension (excessively high blood pressure in the lung arteries), where the right ventricle may be unable to handle the new pressure dynamics after the valve is fixed.
Patients should seek immediate medical attention if they experience:
- Syncope: Fainting spells, which may indicate a dangerous arrhythmia or a sudden drop in oxygen saturation.
- Peripheral Edema: Swelling in the ankles or legs, signaling that the right side of the heart is failing to pump blood efficiently.
- Dyspnea: Shortness of breath during mild activity or while lying flat.
- Palpitations: A fluttering sensation in the chest, often associated with atrial fibrillation in patients with enlarged right atria.
The trajectory for Ebstein Anomaly has shifted from “palliative care” to “functional restoration.” While the condition remains a lifelong challenge, the integration of 3D imaging and the Cone procedure has turned a once-fatal diagnosis into a manageable chronic condition. The future lies in refining the timing of surgery—operating precisely when the heart’s compensatory mechanisms begin to fail, but before the muscle is permanently damaged.