
A recent clinical report highlights the diagnostic challenge of differentiating Eosinophilic Esophagitis (EoE) from Achalasia in young adults. Both conditions present with dysphagia, yet they possess distinct pathophysiologies. Accurate diagnosis requires histological confirmation via esophageal biopsy, as symptoms alone often lead to misdiagnosis, delaying appropriate, targeted therapeutic intervention.
In Plain English: The Clinical Takeaway
- Dysphagia isn’t one-size-fits-all: Difficulty swallowing can stem from immune-driven inflammation (EoE) or nerve-muscle dysfunction (Achalasia).
- Biopsy is the gold standard: You cannot tell these apart by symptoms alone; a tissue sample is required to confirm an eosinophil count.
- Treatment pathways diverge: Using a dilation procedure for inflammation (EoE) without addressing the underlying allergy will not provide long-term relief.
The Diagnostic Overlap: Decoding Dysphagia
In clinical practice, the presentation of progressive dysphagia—difficulty swallowing—in a young adult frequently triggers a broad differential diagnosis. As highlighted in recent literature, the clinical overlap between Eosinophilic Esophagitis (EoE) and Achalasia creates a “diagnostic trap.” EoE is a chronic, immune-mediated esophageal disease characterized by eosinophil-predominant inflammation, whereas Achalasia is a primary esophageal motility disorder caused by the loss of inhibitory neurons in the myenteric plexus.
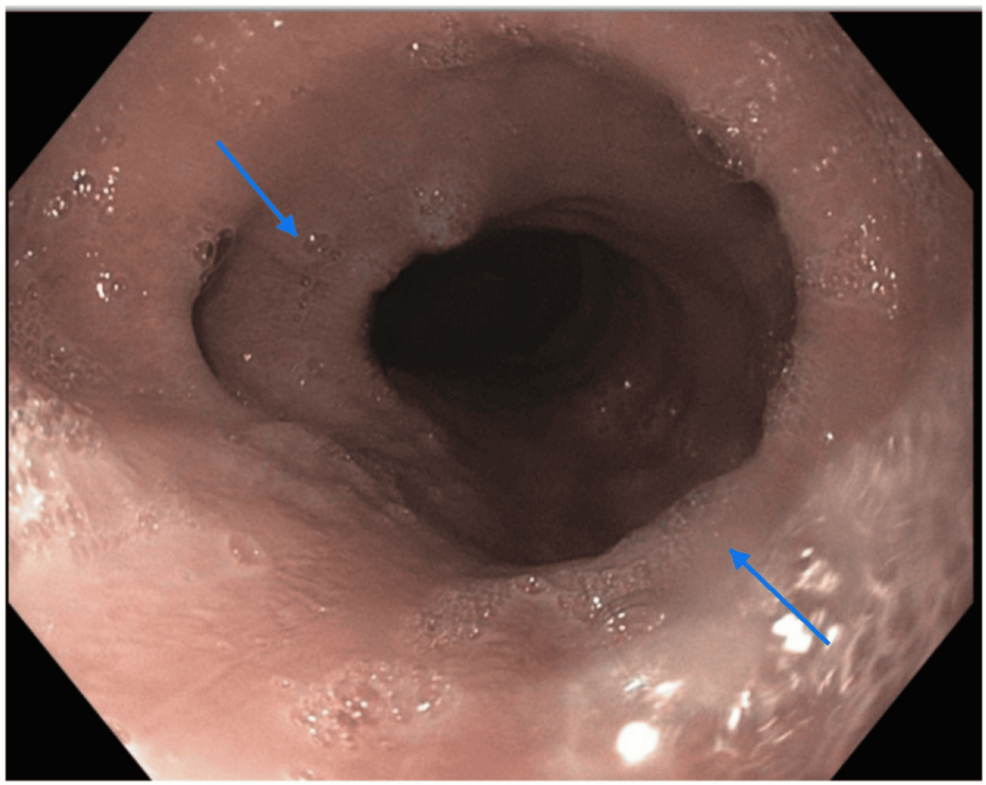
The diagnostic challenge arises because both conditions manifest as food impaction and retrosternal pain. Clinicians must utilize high-resolution manometry (HRM) to assess esophageal pressure and upper endoscopy with biopsy to quantify eosinophil density. Failure to perform these tests in tandem often leads to the misclassification of EoE as Achalasia, particularly when esophageal remodeling results in a narrowed, “bird-beak” appearance on barium swallow imaging.
Clinical Comparison of Esophageal Pathologies
| Feature | Eosinophilic Esophagitis (EoE) | Achalasia |
|---|---|---|
| Primary Mechanism | Allergic/Immune-mediated | Neurodegenerative/Motility |
| Diagnostic Gold Standard | Esophageal biopsy (>15 eos/hpf) | High-resolution manometry (HRM) |
| Common Treatment | Elimination diets, topical steroids | Pneumatic dilation, myotomy |
| Key Morphological Sign | Esophageal rings/furrows | LES failure to relax |
Geo-Epidemiological Considerations and Healthcare Access
The incidence of EoE has risen significantly over the past decade, particularly in Westernized nations. According to data from the Journal of Allergy and Clinical Immunology, this increase is likely linked to environmental factors and shifts in dietary patterns. In the United States, patients navigating the healthcare system often encounter barriers to accessing specialized gastroenterology care, which is necessary for the precise interpretation of HRM studies.
Dr. Evan Dellon, a leading researcher in esophageal diseases, notes that, `The diagnostic delay for patients with EoE often spans several years, as symptoms are frequently attributed to GERD or anxiety. Establishing a definitive diagnosis requires a high index of clinical suspicion, especially when standard acid-suppression therapy fails.` This sentiment is echoed by international consensus, which emphasizes that early histological evaluation is the only way to avoid unnecessary surgical interventions, such as a Heller myotomy, which would be ineffective for an inflammatory condition like EoE.
Contraindications & When to Consult a Doctor
Patients experiencing persistent dysphagia, unintended weight loss, or the sensation of food “sticking” in the chest should not rely on over-the-counter antacids or lifestyle modifications alone. If you have been treated for GERD (Gastroesophageal Reflux Disease) for more than eight weeks without significant symptom resolution, a referral to a gastroenterologist for an esophagogastroduodenoscopy (EGD) is indicated.
Contraindications: Do not attempt aggressive dietary elimination or herbal “cleanses” for dysphagia without medical supervision. In cases of structural narrowing (strictures), self-managed dietary changes can lead to severe food impaction, which is a medical emergency requiring urgent endoscopic removal.
The Future of Precision Esophageal Care
The intersection of these two conditions underscores the necessity of a multidisciplinary approach. As we look toward 2026, the integration of molecular biomarkers and improved imaging protocols will likely reduce the time to diagnosis. For the patient, the “information gap” remains in the understanding that persistent esophageal symptoms are not merely a result of acid reflux but may represent complex, distinct immunological or neurological processes that demand specialized, evidence-based diagnostic rigor.
References
- Dellon ES, et al. “ACG Clinical Guideline: Evidenced Based Approach to the Diagnosis and Management of Esophageal Eosinophilia and Eosinophilic Esophagitis.” American Journal of Gastroenterology.
- Kahrilas PJ, et al. “Achalasia: diagnosis and management.” The Lancet Gastroenterology & Hepatology.
- CDC. “National Health and Nutrition Examination Survey (NHANES) Data Findings.”
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.