
A recent case report published in Cureus highlights the lethal progression of a giant left atrial aneurysm (GLAA), a rare cardiac condition. Complicated by multiple thrombi and resulting in cardiogenic shock, the patient’s rapid decline underscores the critical importance of early diagnostic imaging and surgical intervention for asymptomatic cardiac structural abnormalities.
In Plain English: The Clinical Takeaway
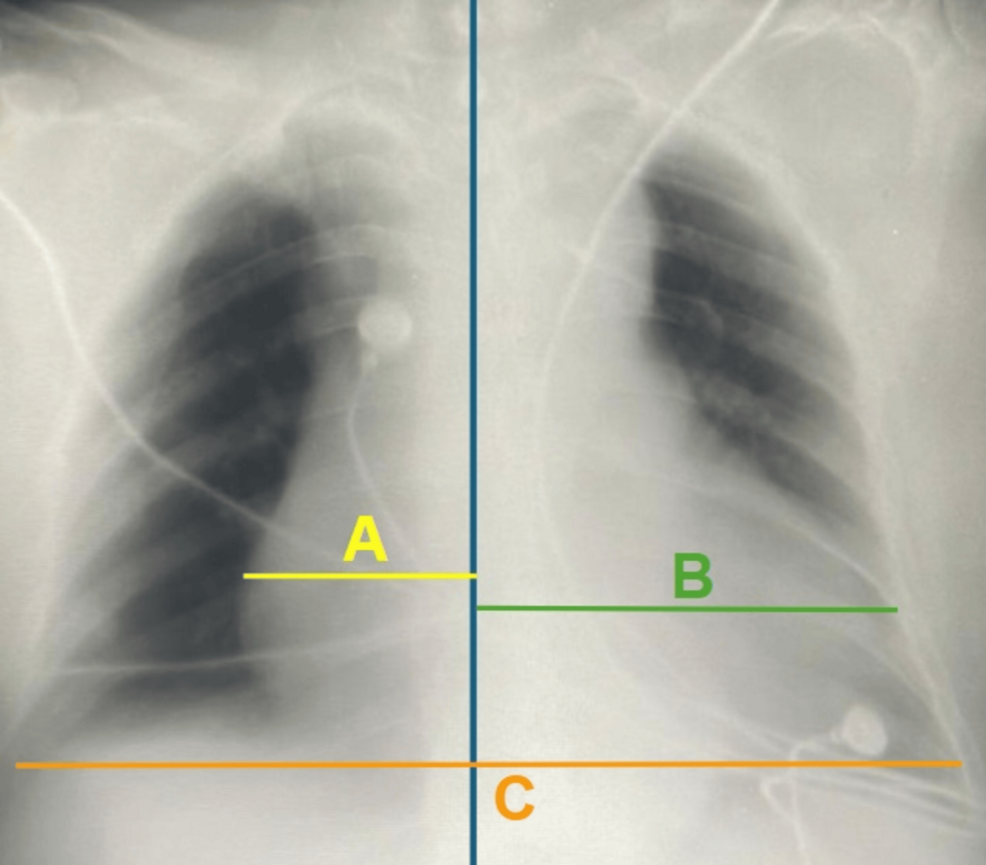
- What is a GLAA? It is an extreme dilation of the left atrium, the chamber of the heart that receives oxygenated blood from the lungs. When it becomes “giant,” it loses the ability to contract effectively, acting as a reservoir for stagnant blood.
- The Thrombus Risk: Because the blood sits still in the enlarged atrium, it clots (thrombi). If these clots break loose, they can travel to the brain (causing a stroke) or further block heart function, as seen in this fatal case.
- The Warning Signs: While often asymptomatic, sudden shortness of breath, palpitations, or unexplained hypotension (low blood pressure) must be treated as a medical emergency requiring urgent echocardiography.
The Pathology of Atrial Stasis and Cardiogenic Collapse
The Cureus report details a scenario where the left atrium, significantly enlarged beyond normal anatomical parameters, failed to maintain hemodynamic stability. In cardiac physiology, the atrium serves as a “primer” for the left ventricle. When an aneurysm occurs—often secondary to mitral valve disease or chronic hypertension—the structural integrity of the atrial wall is compromised. This creates a zone of stasis, or “blood pooling,” which is the primary driver of thrombus formation.
In this specific case, the presence of multiple thrombi created a mechanical obstruction that impaired cardiac output, ultimately leading to cardiogenic shock—a state where the heart is unable to pump sufficient blood to meet the body’s metabolic requirements. As noted by Dr. Robert O. Bonow, a prominent cardiologist, the management of atrial structural pathology requires a high index of suspicion, particularly when patients present with non-specific symptoms that may mask underlying, life-threatening arrhythmias or embolic risks.
Diagnostic and Epidemiological Context
Giant Left Atrial Aneurysm is an exceptionally rare entity. While standard atrial enlargement is common in patients with atrial fibrillation, a “giant” aneurysm is usually defined by a diameter exceeding 6-8 cm. The rarity of the condition often leads to diagnostic delays. Clinical guidelines from the American Heart Association (AHA) emphasize that transthoracic echocardiography (TTE) is the gold standard for initial screening, though transesophageal echocardiography (TEE) is often required to visualize thrombi in the posterior aspect of the left atrium.
The following table summarizes the clinical progression observed in high-risk atrial pathologies:
| Clinical Feature | Pathophysiological Impact | Risk Level |
|---|---|---|
| Atrial Stasis | Promotes Virchow’s Triad (Hypercoagulability) | High |
| Thrombus Formation | Embolic potential (Stroke/Systemic) | Critical |
| Mechanical Obstruction | Impaired ventricular filling | Emergency |
Funding and Research Transparency
This case report was published as an independent medical observation. The authors disclosed no external commercial funding or conflicts of interest. In the broader medical landscape, research into structural heart disease is frequently supported by institutions such as the National Heart, Lung, and Blood Institute (NHLBI). Transparency in these reports is vital to ensure that clinicians do not rely on anecdotal evidence but rather on established surgical protocols when managing rare, high-mortality cardiac events.
Contraindications & When to Consult a Doctor
Patients with a known history of mitral valve regurgitation, chronic atrial fibrillation, or rheumatic heart disease are at the highest risk for progressive atrial dilation. If you experience the following, seek immediate emergency care:
- Sudden onset of severe dyspnea (shortness of breath) while at rest.
- Episodes of syncope (fainting) or near-fainting.
- Persistent, irregular palpitations accompanied by lightheadedness.
There are no “lifestyle” cures for a structural aneurysm of this magnitude; it is a mechanical failure that necessitates clinical evaluation. Patients should not attempt to manage symptoms with over-the-counter anti-platelet agents without explicit direction from a cardiologist, as these do not address the structural source of the risk.
The Future of Surgical Intervention
The tragedy of this case serves as a stark reminder that anatomical heart disease remains a significant cause of mortality. While advanced imaging has improved our ability to detect these aneurysms, the window for surgical intervention—typically involving aneurysmectomy and mitral valve repair—is narrow. Moving forward, clinicians are encouraged to integrate longitudinal monitoring for patients with chronic mitral valve pathology to prevent the silent progression toward a “giant” state.