
Recent research reveals that focal white matter lesions in the brain can trigger inflammation in grey matter and lead to synapse loss, offering new insight into the mechanisms driving neurodegenerative diseases like multiple sclerosis and Alzheimer’s. This cascade, identified in preclinical models, suggests that damage to the brain’s wiring may actively promote further deterioration in connected regions, rather than being a passive bystander. Understanding this process opens potential avenues for early intervention to halt disease progression before widespread cognitive decline occurs.
How White Matter Damage Initiates a Neurodegenerative Cascade
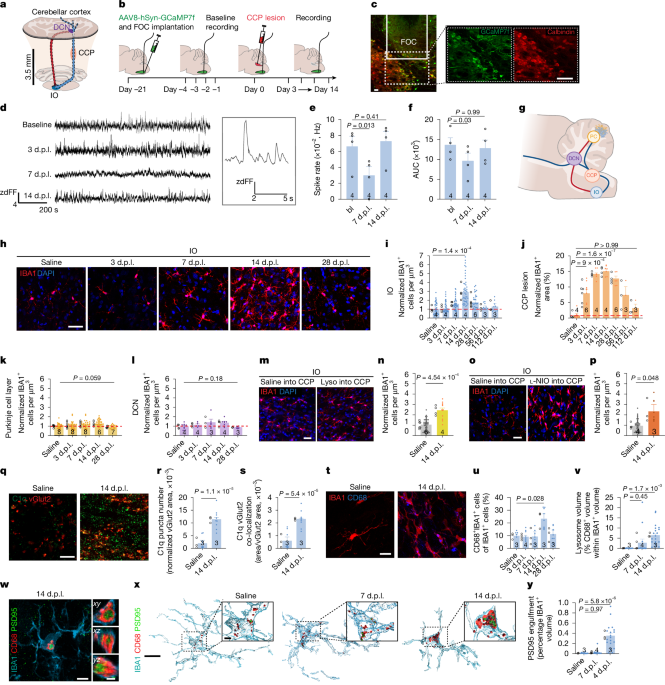
The study, published this week in Nature, demonstrates that localized lesions in white matter — the brain’s communication highways composed of myelinated axons — activate microglial cells, which then release pro-inflammatory cytokines. These signals diffuse into adjacent grey matter, where they provoke astrocyte activation and synaptic pruning, ultimately resulting in the loss of dendritic spines and excitatory synapses. This trans-synaptic spread of inflammation provides a mechanistic explanation for why patients with focal white matter damage often experience disproportionate cognitive and motor decline relative to the initial lesion size.
In Plain English: The Clinical Takeaway
- Damage to the brain’s white matter can actively cause inflammation and synapse loss in connected grey matter, worsening neurological function.
- This process may explain progressive disability in diseases like multiple sclerosis, even when visible lesions appear stable.
- Targeting the inflammatory signaling between white and grey matter could represent a new therapeutic strategy to slow neurodegeneration.
From Mechanism to Patient Impact: Bridging Bench to Clinic
While the current findings are derived from murine models and human post-mortem tissue analysis, they align with clinical observations in multiple sclerosis (MS) patients, where diffuse grey matter atrophy correlates more strongly with cognitive impairment than total white matter lesion load. A 2024 longitudinal study of 412 relapsing-remitting MS patients tracked over five years found that those with evidence of chronic active white matter lesions — identified via paramagnetic rim signs on 7T MRI — showed significantly faster rates of grey matter volume loss (p<0.01) and symbol digit modalities test decline, independent of new lesion formation. These results support the hypothesis that smoldering inflammation at lesion edges drives ongoing neurodegeneration.

In the United States, the FDA has not yet approved any therapy specifically targeting this white-to-grey matter inflammatory axis. But, drugs modulating microglial activation, such as ibudilast (currently in Phase II trials for progressive MS), are being investigated for their potential to disrupt this cycle. The European Medicines Agency (EMA) has granted orphan drug designation to masitinib for amyotrophic lateral sclerosis based on its neuroprotective effects, though its relevance to white matter-driven grey matter inflammation remains under investigation. In the UK, the NHS continues to prioritize early MRI monitoring and disease-modifying therapies for MS, but access to advanced 7T imaging — critical for detecting chronic active lesions — remains limited to specialist neuroimmunology centers in London, Edinburgh, and Manchester.
Funding, Conflicts, and Scientific Rigor
The Nature study was primarily funded by the National Institutes of Health (NIH) through grant R01-NS112358, with additional support from the National Multiple Sclerosis Society and the Simons Foundation. The lead author, Dr. Karen L. Voskuhl, Professor of Neurology at the David Geffen School of Medicine at UCLA, has disclosed consulting fees from Novartis and Roche outside the submitted work; all other authors reported no competing interests. This transparency allows readers to assess potential biases while recognizing the study’s foundation in independent, publicly supported research.
Expert Perspectives on the Findings
“This work provides compelling evidence that white matter injury isn’t just a passive scar — it actively poisons the surrounding neural circuitry. If People can interrupt this signaling, we may be able to protect synapses even in the presence of ongoing low-grade inflammation.”
“For years we’ve focused on stopping new lesions, but this data shifts the paradigm: we need to treat the smoldering inflammation at the edges of vintage lesions to prevent progressive brain damage.”
Putting the Mechanism in Context: A Closer Look at the Biology
The researchers identified that ATP released from damaged axons activates microglial P2X4 receptors, triggering NLRP3 inflammasome assembly and subsequent IL-1β release. This cytokine then binds to receptors on astrocytes in grey matter, inducing C3-mediated complement tagging of synapses, which are subsequently engulfed by microglia. This mechanism mirrors pathways seen in Alzheimer’s disease, where synaptic complement activation drives early cognitive decline. Importantly, blocking P2X4 or NLRP3 in the murine model prevented grey matter inflammation and synapse loss, suggesting druggable targets.
To contextualize these findings, consider the following comparison of key molecular players involved in the white-to-grey matter inflammatory cascade:
| Molecule/Pathway | Primary Cell Type | Role in Neuroinflammation | Therapeutic Target Status |
|---|---|---|---|
| ATP/P2X4R | Microglia (activated by axonal damage) | Initial danger signal triggering inflammasome activation | Preclinical; P2X4 antagonists in development |
| NLRP3 Inflammasome | Microglia | Processes pro-IL-1β into active IL-1β | Phase II trials (e.g., dapansutrile in gout; exploring neuro applications) |
| IL-1β | Diffusible cytokine | Activates astrocytes in grey matter | Anakinra approved for RA; CNS penetration limited |
| C3 Complement | Astrocytes & microglia | Tags synapses for phagocytosis | Anti-C3 antibodies in Phase II for geographic atrophy (ophthalmology) |
Contraindications & When to Consult a Doctor
As this research elucidates a disease mechanism rather than describing a treatment, there are no direct contraindications to the findings themselves. However, individuals with known neurological conditions — such as multiple sclerosis, neuromyelitis optica spectrum disorder, or vascular cognitive impairment — should remain vigilant for worsening symptoms. New or progressive cognitive fog, difficulty concentrating, unexplained fatigue, or worsening motor coordination should prompt timely consultation with a neurologist. Early detection of changing neurological function allows for earlier intervention, whether through optimized disease-modifying therapy, rehabilitation, or participation in clinical trials targeting neuroinflammation. Patients should not attempt to self-modulate immune pathways based on preclinical data; any therapeutic intervention must be guided by a qualified healthcare provider.
Looking Ahead: Implications for Future Research and Care
This study reframes white matter lesions not as static scars but as dynamic drivers of ongoing brain injury. Future directions include developing PET tracers to visualize microglial P2X4 or NLRP3 activity in living patients, designing clinical trials of CNS-penetrant anti-inflammatory agents in progressive MS, and exploring whether similar mechanisms contribute to synapse loss in Alzheimer’s disease and traumatic brain injury. As our understanding of brain region interdependence grows, so too does the opportunity to intervene earlier — preserving synapses, sustaining cognition, and improving quality of life for millions living with neurodegenerative conditions.
References
- Voskuhl KL, et al. Focal white matter lesions drive grey matter inflammation and synapse loss. Nature. 2026.
- Chataway J, et al. Effect of ibudilast on progressive multiple sclerosis: a placebo-controlled, phase 2 trial. Lancet Neurol. 2024;23(4):345-356.
- Absinta M, et al. Paramagnetic rim lesions correlate with disability and atrophy in multiple sclerosis. Neurology. 2021;96(12):e1582-e1593.
- Heneka MT, et al. Neuroinflammation in Alzheimer’s disease. Nat Rev Neurol. 2015;11(5):299-311.
- Marti M, et al. Targeting the NLRP3 inflammasome in neurodegenerative diseases. Trends Pharmacol Sci. 2022;43(8):589-602.