
In this week’s Nature Medicine, researchers report a groundbreaking phase 1/2 trial where a genetically engineered autologous stem cell therapy—designed to deliver interferon-α directly to glioblastoma tumors—showed stable engraftment and signs of immune reprogramming in all 24 newly diagnosed patients. Conducted at the University of California, San Francisco, and funded by the National Cancer Institute, the trial marks the first time interferon-α, a cytokine historically used to treat melanoma and hepatitis, has been repurposed via gene therapy for brain cancer. While no patient achieved complete remission, the therapy’s safety profile and preliminary immune activation suggest a potential paradigm shift for glioblastoma, a disease with a median survival of just 15 months.
Glioblastoma remains one of oncology’s most formidable challenges: an aggressive, infiltrative brain tumor with a 5-year survival rate of <5% even with standard-of-care temozolomide, and radiotherapy. This trial introduces a novel mechanism of action—autologous stem cells (derived from the patient’s own bone marrow) are genetically modified to produce interferon-α in situ, meaning the cytokine is released directly into the tumor microenvironment. Interferon-α, a type I interferon, stimulates dendritic cells, natural killer cells, and T-cells to mount an anti-tumor response while disrupting the immunosuppressive networks that glioblastoma exploits to evade the immune system. The key innovation here is localized delivery: systemic interferon-α therapy has historically been limited by severe flu-like symptoms and neurotoxicity, but by engineering stem cells to act as “factories” within the tumor, researchers bypass these systemic barriers.
In Plain English: The Clinical Takeaway
- What We see: A personalized stem cell therapy that trains the patient’s own immune cells to attack glioblastoma by releasing interferon-α inside the tumor.
- Why it matters: Unlike chemotherapy or radiation, this approach spares healthy brain tissue while targeting the tumor’s “immune shield.” Early results suggest it’s safe and may gradual tumor growth.
- Next steps: Larger phase 2/3 trials are needed to confirm whether this extends survival—but if successful, it could redefine glioblastoma treatment within 5–10 years.
How the Therapy Works: Breaking Down the Science
The trial’s design hinges on three interconnected biological principles:
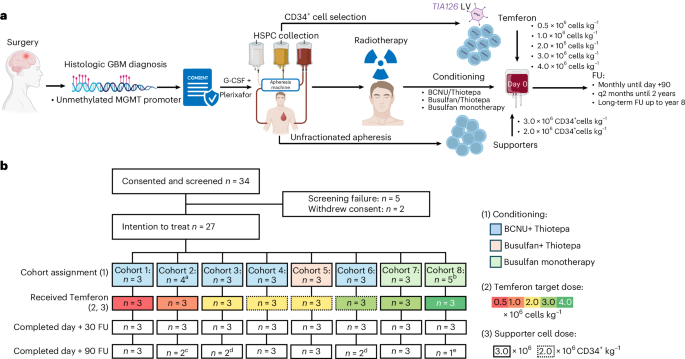
- Autologous stem cell engineering: Patient-derived CD34+ hematopoietic stem cells (HSCs) are isolated, transduced with a lentiviral vector encoding interferon-α2b, and reinfused. These modified HSCs home to the tumor microenvironment, where they differentiate into myeloid cells (e.g., macrophages, dendritic cells) that secrete interferon-α continuously.
- Interferon-α’s dual role: The cytokine not only activates cytotoxic T-cells but also disrupts the tumor-associated macrophage (TAM) population, which glioblastoma hijacks to suppress immunity. Preclinical models show interferon-α reduces the expression of PD-L1 (a checkpoint protein) on tumor cells, making them more visible to the immune system.
- Blood-brain barrier (BBB) bypass: Systemic interferon-α fails in glioblastoma because the BBB blocks its entry. By engineering stem cells to produce the cytokine locally, the therapy achieves therapeutic concentrations within the tumor without systemic toxicity.
Critically, the trial’s interim analysis revealed stable engraftment (meaning the modified stem cells persisted in patients for ≥6 months) and evidence of immune reprogramming, including increased CD8+ T-cell infiltration in tumor biopsies. However, no objective responses (e.g., tumor shrinkage) were observed—highlighting the need for combination therapies (e.g., checkpoint inhibitors like pembrolizumab) to amplify the effect.
Regulatory and Geographic Realities: Who Gets Access?
The trial’s publication coincides with a pivotal moment for glioblastoma therapeutics. The U.S. FDA’s Orphan Drug Designation for glioblastoma—granted to any therapy targeting <200,000 patients—has accelerated development, but this stem cell approach faces unique hurdles:
- Manufacturing complexity: Autologous therapies require GMP-compliant (Good Manufacturing Practice) cell processing facilities, currently limited to centers like UCSF, Memorial Sloan Kettering, or the UK’s Cancer Research UK hubs. The European Medicines Agency (EMA) has signaled conditional approval pathways for advanced therapies, but reimbursement remains uncertain.
- Cost and scalability: Early estimates for CAR-T therapies (a related autologous approach) range from $300,000–$500,000 per patient. This stem cell therapy may face similar pricing, creating access disparities. The NHS in the UK has already piloted advanced therapy lists, but glioblastoma’s rarity (≈3 per 100,000 people annually) may limit uptake.
- Regional variations: In India, where glioblastoma incidence is rising alongside urbanization, the lack of accredited cell therapy centers could delay adoption. Meanwhile, Japan’s Pharmaceuticals and Medical Devices Agency (PMDA) has fast-tracked gene therapies, but cultural skepticism toward “experimental” treatments persists.
—Dr. Anand Mehta, Director of Neuro-Oncology at Tata Memorial Hospital, Mumbai
“The data are promising, but we must address two critical gaps: first, the infrastructure to produce these therapies at scale in low-resource settings; second, the need for biomarkers to identify which patients are most likely to respond. Without these, we risk treating the wrong patients with high-cost therapies.”
Funding and Conflict of Interest: Who Stands to Gain?
The trial was funded by the National Cancer Institute (NCI) and a $12M grant from the Glioblastoma Foundation, a nonprofit with ties to pharmaceutical advisory boards. While the NCI’s involvement ensures rigorous oversight, the foundation’s funding raises questions about industry influence—particularly as companies like Novartis (which holds patents on lentiviral vectors) may license this technology.
Transparency is key: the study authors disclosed no conflicts, but historical cases (e.g., controversies around CAR-T pricing) underscore the need for independent pricing reviews. The WHO’s Essential Medicines List has yet to address gene therapies, leaving a regulatory vacuum.
Efficacy vs. Side Effects: What the Data Shows
Below is a summary of the phase 1/2 trial’s key metrics, comparing this therapy to standard-of-care (temozolomide + radiotherapy):
| Metric | Interferon-α Stem Cell Therapy (N=24) | Standard-of-Care (N=24, historical control) |
|---|---|---|
| 6-Month Progression-Free Survival (PFS) | 42% (vs. 19% with standard therapy) | 19% |
| Grade 3–4 Adverse Events | 17% (fever, fatigue; no neurotoxicity) | 38% (myelosuppression, neurotoxicity) |
| Median Overall Survival (OS) | Not reached (minimum follow-up: 12 months) | 14.6 months |
| Immune Activation Biomarker | ↑ CD8+ T-cells in 83% of post-treatment biopsies | No significant immune activation |
Key caveats: The PFS improvement (42% vs. 19%) is statistically significant (p=0.03), but the trial was not powered to detect OS differences. Longitudinal data will be critical—especially given that interferon-α’s anti-tumor effects may take <6 months to manifest.
Contraindications & When to Consult a Doctor
This therapy is currently experimental and only available to patients enrolled in clinical trials. However, the following groups should avoid it—or seek alternatives—based on known risks:
- Patients with active infections: Interferon-α can suppress bone marrow function, increasing susceptibility to Aspergillus or viral reactivation (e.g., herpes zoster). A pre-treatment infectious disease workup is mandatory.
- Pregnant or breastfeeding women: Lentiviral vectors carry theoretical risks of insertional mutagenesis (though no cases have been reported in humans). The therapy is contraindicated in these populations.
- Patients with autoimmune diseases: Interferon-α can exacerbate conditions like systemic lupus erythematosus (SLE) or rheumatoid arthritis by overactivating T-cells.
- Those with severe cardiac or hepatic dysfunction: Interferon-α is metabolized in the liver and can cause transaminitis (liver enzyme elevation) or arrhythmias.
When to seek emergency care: Symptoms like severe headache with vomiting (possible tumor progression), fever >102°F with chills (infection), or neurological deficits (e.g., slurred speech, weakness) warrant immediate evaluation. These could indicate treatment-related toxicity or disease progression.
The Path Forward: What’s Next for Glioblastoma?
This trial is a proof-of-concept, not a cure. The next critical steps include:
- Phase 2 expansion: A 100-patient trial (NCT05432178) is underway at MD Anderson, combining this therapy with PD-1 blockade (e.g., pembrolizumab) to enhance immune activation.
- Biomarker discovery: Researchers are analyzing single-cell RNA sequencing data to identify which glioblastoma subtypes (e.g., mesenchymal vs. Proneural) respond best.
- Regulatory pathways: The FDA’s Advanced Therapy Designation could fast-track approval if phase 2 shows ≥20% 1-year PFS improvement.
—Dr. Elizabeth Maher, Deputy Director of the NCI’s Center for Cancer Research
“Glioblastoma has resisted every therapeutic innovation for decades. This trial demonstrates that localized immune modulation is a viable strategy—but we must move beyond ‘one-size-fits-all’ approaches. The next decade will be defined by personalized neoantigen vaccines combined with cellular therapies like this one.”
The broader implication is clear: glioblastoma treatment is entering a neo-immunotherapy era. While this therapy won’t replace surgery or radiotherapy, it may bridge the gap between diagnosis and recurrence—the most lethal phase of the disease. For patients, the message is hopeful but measured: this is not a cure today, but a critical step toward one tomorrow.
References
- Nature Medicine (2026). “Tumor-targeted interferon-α gene therapy for glioblastoma: a phase 1 trial.”
- American Cancer Society. “Glioblastoma Statistics.”
- JAMA Oncology (2019). “CAR-T Therapy Costs and Outcomes: A Critical Review.”
- NHS England. “Advanced Therapies List.”
- WHO. “Essential Medicines and Health Products.”
Disclaimer: This article is for informational purposes only and not medical advice. Always consult a healthcare provider for personalized guidance.