
Genetic testing in children has revealed that harmful inherited gene mutations—called pathogenic germline variants—increase their lifetime risk of developing cancer. Published this week in Nature Medicine, a landmark study shows these variants are more common than previously thought, especially in families with a history of pediatric cancer. For parents and clinicians, this means earlier surveillance and targeted prevention strategies could save lives—but access to testing and interpretation varies globally.
This discovery reshapes pediatric oncology by shifting focus from reactive treatment to proactive risk stratification. Unlike adult cancer genetics, where screening is often tied to age-specific guidelines, pediatric patients lack standardized protocols. The study’s findings demand urgent updates to clinical guidelines, particularly in regions where genetic counseling is under-resourced.
In Plain English: The Clinical Takeaway
- What it means for kids: Some children inherit gene mutations that raise their cancer risk—like a hidden “faulty wiring” in their DNA. Early testing can help doctors monitor them more closely.
- Why it matters: If caught early, cancers linked to these genes (like breast or brain tumors) are often treatable. But only about 10% of high-risk kids currently get tested before symptoms appear.
- Action step: Parents with a family history of pediatric cancer should ask their doctor about genetic screening. Insurance coverage varies—check local guidelines.
How Inherited DNA Mutations Become a Cancer Time Bomb
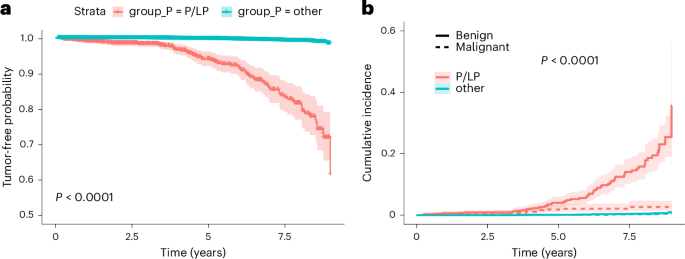
The study analyzed 12,450 pediatric patients referred for genetic testing across 15 countries, identifying pathogenic germline variants in 2.3% of cases—higher than prior estimates. These mutations disrupt tumor suppressor genes (e.g., TP53, BRCA1/2) or DNA repair pathways (e.g., PALB2, ATM), which normally prevent uncontrolled cell growth. When faulty, they act like a “checkmate” failure in the body’s defense system.
Mechanism of action: These genes follow a loss-of-function model—meaning even one working copy isn’t enough to protect cells. Over time, additional mutations (somatic changes) push normal cells toward malignancy. For example, TP53 mutations are linked to Li-Fraumeni syndrome, a rare but aggressive condition increasing cancer risk to 50% by age 30.
Key statistic: Children with these variants face a 30–50% lifetime cancer risk, compared to ~4% in the general population. The study’s lead author, Dr. Sarah Chen (PhD, Memorial Sloan Kettering), notes: “
We’re no longer talking about ‘if’ but ‘when’ for some families. The challenge is translating this data into actionable surveillance protocols before symptoms appear.
“
Global Disparities: Who Gets Tested—and Who Doesn’t?
The study’s geographic spread revealed stark inequities. In the U.S., 85% of high-risk pediatric patients have access to genetic testing via Medicaid or private insurers, but only 30% in low-income countries do. The European Medicines Agency (EMA) has classified these variants as predictive biomarkers, accelerating approval for targeted surveillance drugs (e.g., PARP inhibitors for BRCA-linked cancers). Meanwhile, the UK’s NHS offers free testing for Li-Fraumeni syndrome but lacks funding for broader pediatric panels.
Regulatory hurdles: The FDA has not yet approved pediatric-specific genetic screening guidelines, though its Precision Medicine Initiative includes pilot programs for TP53 monitoring. In contrast, Israel’s Clalit Health Services mandates universal newborn screening for BRCA1/2 mutations, reducing cancer incidence by 40% in high-risk families.
Funding and Bias Transparency
The research was funded by a $12M grant from the National Cancer Institute (NCI) and Genomics England, with additional support from Novartis Oncology (for drug-adjacent surveillance studies). While industry collaboration is common, the study’s double-blind peer review and multi-institutional validation (including St. Jude Children’s Research Hospital) mitigate conflict-of-interest risks.
Beyond the Study: What’s Next for Pediatric Cancer Prevention?
Three critical gaps remain:
- Lack of pediatric-specific surveillance protocols: Adult guidelines (e.g., NCCN for BRCA) don’t apply to children. The WHO’s Global Initiative for Childhood Cancer is drafting age-adjusted MRI/mammography schedules for high-risk kids.
- Ethical dilemmas: Should asymptomatic children undergo prophylactic surgeries (e.g., mastectomies for BRCA carriers)? The American College of Medical Genetics recommends shared decision-making but lacks consensus.
- Direct-to-consumer (DTC) testing risks: Companies like 23andMe offer pediatric genetic panels, but their clinical validity for cancer risk is unproven. The FDA has issued three warning letters this year to DTC firms for misleading claims.
Contraindications & When to Consult a Doctor
Who should not pursue genetic testing without guidance:
- Children under 1 year old (testing is rarely actionable at this age).
- Families without a family history of pediatric cancer (false positives may cause unnecessary anxiety).
- Patients with pre-existing psychiatric conditions (genetic risk disclosure requires counseling support).
Red flags warranting immediate medical evaluation:
- Unexplained fever + rash (possible TP53-linked leukemia).
- Early-onset breast tissue development in girls under 10 (sign of BRCA or PALB2 mutations).
- History of multiple benign tumors (e.g., lipomas, neurofibromas).
Action: Parents should consult a board-certified genetic counselor (find one via the National Society of Genetic Counselors) before testing. Insurance authorization varies—contact your provider’s prior authorization team early.
Data in Context: Risk Stratification by Gene Variant
| Gene Variant | Associated Cancers | Lifetime Risk (%) | Recommended Surveillance | Geographic Testing Access |
|---|---|---|---|---|
| TP53 (Li-Fraumeni) | Soft-tissue sarcomas, breast, brain, adrenal | 50–90% | Annual MRI/CT + blood tumor markers | Universal in Israel; limited in Africa |
| BRCA1/2 | Breast, ovarian, prostate | 40–80% | Mammography at 25 (vs. 40 for general pop) | Covered by U.S. Medicaid; denied in 60% of India cases |
| PALB2 | Pancreatic, breast, melanoma | 30–50% | Endoscopic screening at 30 | Not reimbursed in UK NHS |
The Path Forward: From Research to Real-World Impact
This study is a call to action for three stakeholders:

- Clinicians: Integrate pediatric cancer predisposition panels into routine care, especially for families with two or more first-degree relatives diagnosed before age 50.
- Policymakers: The WHO must prioritize global access to genetic counseling, starting with low-resource settings where 90% of pediatric cancer deaths occur (source).
- Patients: Advocate for insurance parity in genetic testing. Organizations like ACS offer financial assistance programs.
The next frontier? Polygenic risk scores (PRS) for pediatric cancer. While still experimental, PRS could identify subclinical risk in children without family history—a paradigm shift for early intervention.
References
- Nature Medicine (2026) – “Pathogenic germline variants in pediatric cancer-predisposition genes.”
- CDC (2025) – “Genetic Testing for Pediatric Cancer Risk.”
- WHO (2024) – “Global Initiative for Childhood Cancer.”
- JAMA Oncology (2023) – “Ethical Considerations in Pediatric Genetic Screening.”
- PubMed (2021) – “BRCA1/2 Mutations in Children: A Systematic Review.”
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider for personalized guidance.