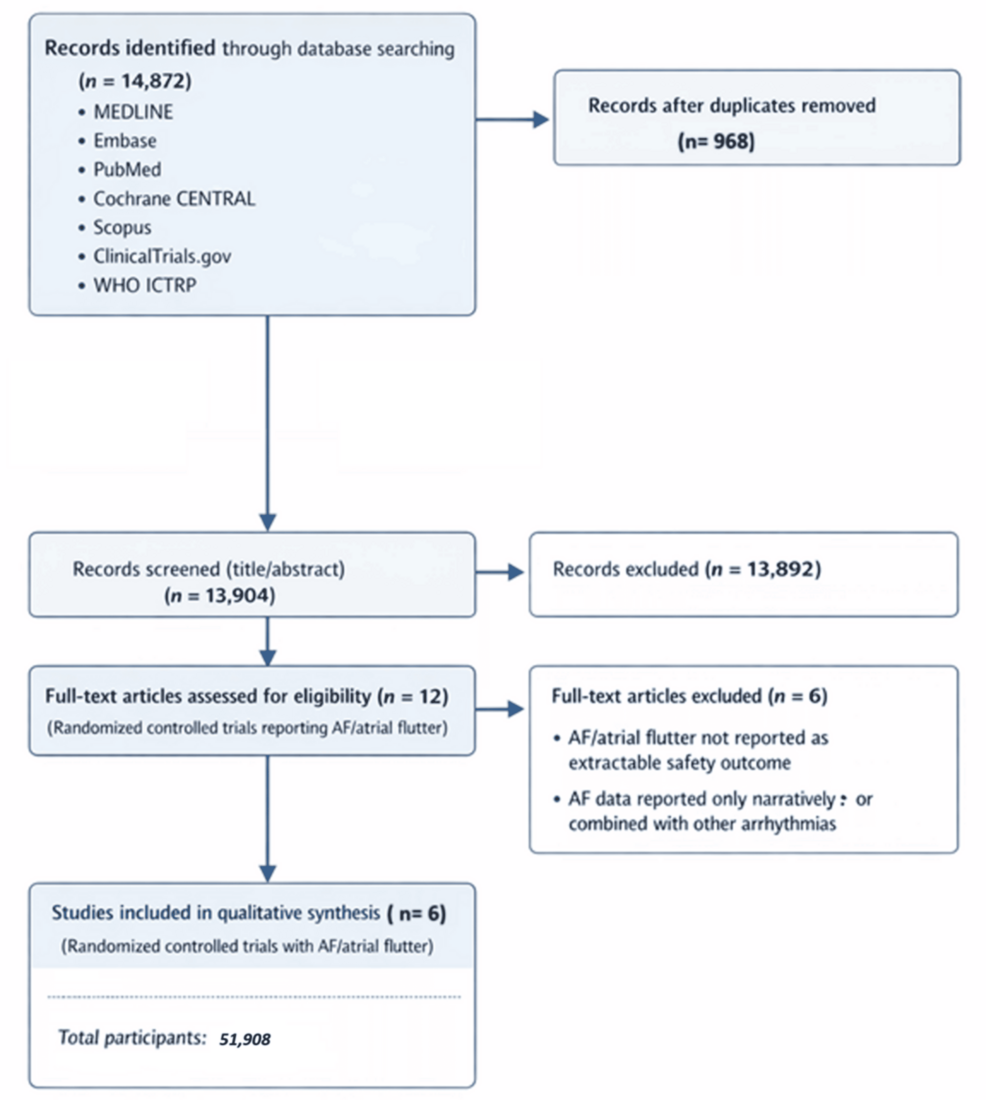
This week, a comprehensive analysis published in Cureus examined whether glucagon-like peptide-1 (GLP-1) receptor agonists—medications widely used for type 2 diabetes and obesity—are associated with an increased risk of atrial fibrillation, a common heart rhythm disorder. The review synthesized data from multiple randomized controlled trials to assess cardiovascular safety signals in patients using these drugs. While GLP-1 receptor agonists have demonstrated significant benefits in glycemic control and weight reduction, concerns about potential arrhythmic effects have prompted closer scrutiny from regulators and clinicians alike. Understanding this association is critical for informing prescribing practices, particularly in patients with pre-existing cardiac risk factors.
In Plain English: The Clinical Takeaway
Current evidence does not show a clear, consistent increase in atrial fibrillation risk from GLP-1 receptor agonists across major trials.
Any potential signal remains uncertain and may be influenced by study design, patient populations, or duration of exposure.
Patients should not discontinue prescribed GLP-1 therapy without consulting their healthcare provider, as benefits often outweigh unproven risks.
Mechanistic Plausibility and Cardiovascular Interactions
GLP-1 receptor agonists, such as semaglutide and liraglutide, enhance insulin secretion, suppress glucagon release and slow gastric emptying through activation of the GLP-1 receptor—a target found not only in pancreatic beta cells but also in the heart, vasculature, and central nervous system. While these drugs improve metabolic parameters and have demonstrated reductions in major adverse cardiovascular events (MACE) in trials like LEADER and SUSTAIN-6, their direct electrophysiological effects on cardiac tissue remain incompletely understood. Some preclinical studies suggest GLP-1 signaling may modulate autonomic tone or influence atrial fibrosis, potentially creating a substrate for arrhythmias under certain conditions. However, human data linking receptor activation to ectopic atrial activity or re-entrant circuits remain inconclusive, underscoring the need for dedicated electrophysiological monitoring in future trials.
In the United States, the FDA continues to monitor post-marketing safety data for GLP-1 receptor agonists through the Adverse Event Reporting System (FAERS), though no formal label changes regarding atrial fibrillation risk have been issued as of early 2026. The European Medicines Agency (EMA) similarly maintains that the benefit-risk balance remains favorable, particularly for patients with established cardiovascular disease. In the UK, the NHS has expanded access to semaglutide for weight management in specialized tiers, but clinicians are advised to assess baseline cardiac history—including prior arrhythmias—before initiation. These regional approaches reflect a shared emphasis on individualized risk assessment rather than population-wide restrictions, acknowledging both the therapeutic value and the evolving safety profile of this drug class.
Funding Sources and Research Independence
The systematic review and meta-analysis published in Cureus received no direct industry funding, according to the authors’ conflict-of-interest statement. Instead, the research was conducted independently by academic clinicians affiliated with a university medical center, with support limited to institutional resources. This absence of pharmaceutical sponsorship strengthens the credibility of the findings, particularly given the heightened scrutiny around industry-backed analyses in metabolic therapeutics. Transparency in funding is essential when evaluating safety signals, as financial ties can inadvertently influence study design, outcome selection, or interpretation—especially in areas where signal detection is nuanced and event rates are low.
Expert Perspectives on Clinical Interpretation
“While mechanistic plausibility exists for GLP-1 receptor agonists to influence atrial electrophysiology, current clinical evidence does not support a causal relationship with atrial fibrillation. Observed signals in some trials may reflect confounding factors such as baseline risk, concomitant medications, or surveillance bias rather than a direct drug effect.”
“Regulatory decisions must be based on robust, reproducible data. Until we observe consistent signals across large, long-term outcome trials with dedicated arrhythmia monitoring, we should avoid overinterpreting isolated adverse event reports. The priority remains ensuring patients with diabetes and obesity aren’t denied effective therapies due to theoretical concerns.”
Key Trial Data Summary
Trial
Drug
Population (N)
Duration
AF Events (Drug vs. Placebo)
LEADER
Liraglutide
9,340
3–5 years
68 vs. 62
SUSTAIN-6
Semaglutide
3,298
2 years
28 vs. 24
PIONEER 6
Oral semaglutide
3,183
15–18 months
19 vs. 17
SELECT (interim)
Semaglutide
17,604
Ongoing
Not yet published for AF-specific analysis
Contraindications & When to Consult a Doctor
GLP-1 receptor agonists are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 (MEN 2), due to observed thyroid C-cell tumors in rodent studies. They should be used with caution in individuals with a history of pancreatitis, severe gastrointestinal disease, or renal impairment. Patients experiencing new-onset palpitations, irregular heartbeat, dizziness, or chest discomfort after initiating therapy should seek prompt medical evaluation, as these may signal arrhythmia or other cardiac events requiring ECG monitoring. Importantly, symptoms such as mild nausea or decreased appetite during dose titration are common and expected but should be distinguished from cardiovascular warning signs. Any concern about heart rhythm changes warrants consultation with a healthcare provider—never self-discontinuation without guidance.
Receptor Agonists Patients Cardiovascular
As real-world usage of GLP-1 receptor agonists expands beyond diabetes into obesity management and cardiovascular risk reduction, ongoing vigilance is essential. Future research must incorporate standardized arrhythmia detection—such as intermittent ECG monitoring or implantable loop recorders—to definitively assess long-term electrophysiological safety. Until then, clinicians are advised to weigh proven benefits against theoretical risks, prioritize patient-specific factors, and maintain open dialogue about both therapeutic promise, and uncertainty.
References
Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2016. 375(4):311-322. Doi:10.1056/NEJMoa1603827
Marso SP, Bain SC, Consoli A, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2016;375(18):1734-1744. Doi:10.1056/NEJMoa1607141
Gerstein HC, Colhoun HM, Dagenais GR, et al. Cardiovascular and Microvascular Outcomes with Semaglutide in Patients with Type 2 Diabetes (PIONEER 6). Lancet. 2019;394(10200):847-856. Doi:10.1016/S0140-6736(19)31750-5
FDA. Adverse Event Reporting System (FAERS) Public Dashboard. Accessed April 2026. Https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html
EMA. Guideline on the clinical investigation of medicinal products for the treatment of diabetes mellitus. 2023. Https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-diabetes-mellitus_en.pdf
Dr. Priya Deshmukh
Senior Editor, Health
Dr. Deshmukh is a practicing physician and renowned medical journalist, honored for her investigative reporting on public health. She is dedicated to delivering accurate, evidence-based coverage on health, wellness, and medical innovations.