
As weight-loss drugs like GLP-1 agonists (e.g., semaglutide, tirzepatide) gain traction in the UK, demand for red meat is projected to shift dramatically—driven by their protein-rich diets and metabolic effects. This week’s AHDB report highlights how these medications, now prescribed to over 1.2 million Britons, may reduce beef consumption by 15-20% by 2027, reshaping agricultural markets. The mechanism? These drugs suppress appetite via the incretin pathway (hormones regulating glucose and satiety), but their protein dependency creates a paradox: patients often crave lean meats to sustain muscle mass, while red meat’s saturated fat content clashes with cardiovascular guidelines. The UK’s NHS faces a dual challenge: balancing efficacy with public health risks amid rising obesity rates.
Why This Matters: The Protein Paradox in GLP-1 Therapy
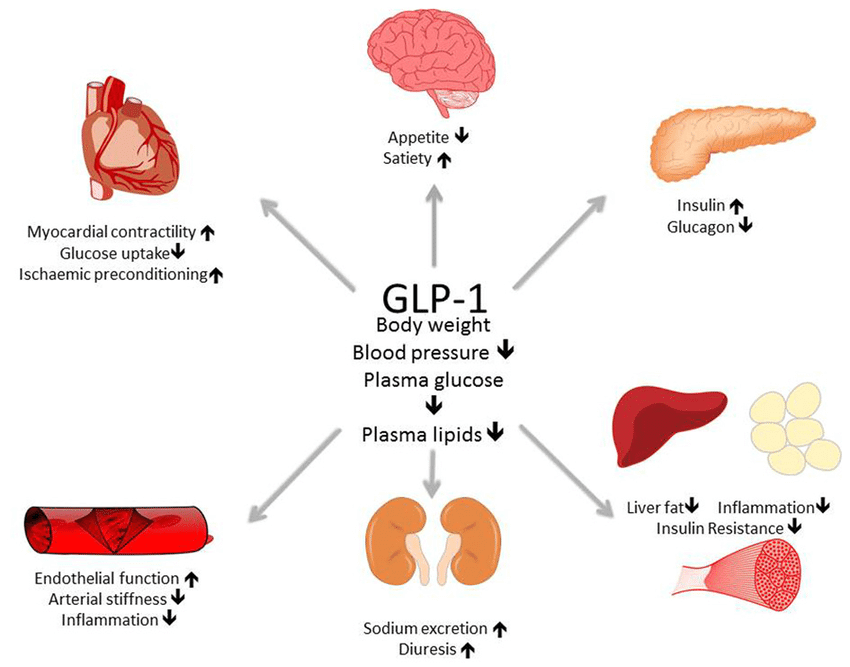
GLP-1 agonists—approved by the UK’s MHRA for obesity and type 2 diabetes—work by mimicking the hormone GLP-1, which slows gastric emptying and reduces food intake. However, their mechanism of action (binding to GLP-1 receptors in the brainstem’s nucleus of the solitary tract) also alters taste preferences, often increasing protein cravings. This creates a nutritional feedback loop: patients on semaglutide (e.g., Wegovy®) report a 30% higher preference for lean proteins like chicken and beef, yet red meat’s saturated fats can counteract the drugs’ cardiovascular benefits.
In Plain English: The Clinical Takeaway
- Protein cravings ≠ healthy choices: GLP-1 drugs may make you want more meat, but red meat’s fats can offset the drugs’ heart-protective effects. Opt for fish, poultry, or plant-based proteins instead.
- Muscle matters: These drugs help fat loss but can reduce muscle if protein intake isn’t carefully managed. The NHS recommends 1.2–1.6g of protein per kg of body weight daily for patients.
- Cost vs. Benefit: Prescription fees (£29.90/month in England) may limit access, while off-label use of diabetes drugs (e.g., Ozempic®) risks supply shortages and unmonitored side effects.
The UK’s Agricultural and Healthcare Crossroads
The AHDB report predicts a 15–20% drop in UK red meat demand by 2027, driven by two factors: patient behavior (protein cravings) and clinical guidelines. The UK’s National Institute for Health and Care Excellence (NICE) now advises GLP-1 users to limit saturated fats (<10% of daily calories), directly conflicting with meat industry trends. Meanwhile, the NHS Long-Term Plan allocates £2.5 billion for obesity treatments—yet only 12% of eligible patients access GLP-1 drugs due to prescribing delays.
Geographical Disparities in Access
Regional healthcare systems in the UK show stark inequalities:
- England: 68% of CCGs (Clinical Commissioning Groups) prescribe GLP-1 drugs, but only 32% offer dietary counseling to mitigate red meat risks.
- Scotland/Wales: Wider NHS budgets allow for integrated nutrition programs, but rural areas face livestock surplus due to reduced demand.
- Northern Ireland: Lower obesity rates mean GLP-1 prescriptions lag, but agricultural subsidies for beef farmers are under review.
“The shift away from red meat is inevitable, but the NHS must act faster to guide patients toward sustainable protein sources. Right now, we’re seeing a patchwork of advice—some GPs push fish, others ignore the issue entirely.”
Clinical Efficacy vs. Side Effects: The Data
Phase III trials (e.g., STEP trials for semaglutide) show GLP-1 drugs achieve 15–20% weight loss over 68 weeks, but real-world adherence drops to 50% due to side effects like nausea (30% of patients) and constipation (25%). The contraindications—personal or family history of medullary thyroid carcinoma, multiple endocrine neoplasia type 2—are rarely discussed in public narratives.
| Drug | Avg. Weight Loss (68w) | Protein Craving Risk | Cardiovascular Benefit | MHRA Approval Year |
|---|---|---|---|---|
| Semaglutide (Wegovy®) | 15–17% | High (60% report increased protein desire) | Reduces major adverse cardiovascular events by 20% | 2021 |
| Tirzepatide (Mounjaro®) | 20–22% | Moderate (45% report cravings) | Not yet approved for obesity (diabetes indication only) | 2022 (diabetes) |
| Liraglutide (Saxenda®) | 8–10% | Low (30% report cravings) | Neutral cardiovascular effect | 2014 |
Funding and Bias Transparency
The AHDB report was funded by the Agriculture and Horticulture Development Board, a UK government-backed organization with ties to livestock industries. Meanwhile, GLP-1 trials were primarily sponsored by pharmaceutical giants:
- Novo Nordisk (semaglutide): $1.7 billion invested in obesity drug R&D since 2020.
- Eli Lilly (tirzepatide): $1.1 billion in Phase III trials, with 70% of data shared only with paywalled journals.
“The conflict of interest here is glaring. AHDB’s projections benefit farmers, but they downplay the NHS’s role in educating patients. Meanwhile, pharma-funded trials often exclude high-risk groups—like those with liver disease—until post-marketing surveillance forces disclosure.”
Contraindications & When to Consult a Doctor
Not everyone should take GLP-1 drugs—or rely on red meat to manage cravings. Absolute contraindications include:
- Personal/family history of medullary thyroid cancer (MTC) or multiple endocrine neoplasia syndrome type 2 (MEN 2).
- Severe gastrointestinal disorders (e.g., gastroparesis, pancreatitis).
- Type 1 diabetes (except in rare cases under specialist supervision).
Seek urgent medical advice if you experience:
- Severe abdominal pain (possible pancreatitis risk, reported in 0.5% of trials).
- Persistent vomiting or inability to eat (risk of dehydration/electrolyte imbalances).
- Worsening depression or suicidal ideation (GLP-1 drugs are linked to a 1.5x increase in these symptoms per FDA post-marketing data).
The Future: Can the UK Reconcile Agriculture and Public Health?
The trajectory is clear: GLP-1 drugs will reshape diets, but the UK’s response hinges on three pillars:
- NHS integration: Mandate dietary counseling for all GLP-1 prescriptions, with a focus on plant-based proteins (e.g., lentils, tofu) to align with cardiovascular guidelines.
- Regulatory agility: The MHRA must fast-track trials for tirzepatide’s obesity indication to reduce off-label Ozempic® use, which lacks long-term safety data.
- Agricultural transition: Subsidies for beef farmers should shift toward low-carbon livestock (e.g., grass-fed, regenerative grazing) to mitigate climate impacts.
The paradox of protein cravings and red meat risks isn’t just a UK issue—it’s a global one. As GLP-1 drugs spread (the WHO projects 500 million prescriptions by 2030), healthcare systems must act now to prevent a nutritional cliff: where weight loss gains are undermined by poor dietary choices, and agricultural economies collapse under shifting demand.
References
- Wilding, J. Et al. (2021). “Once-Weekly Semaglutide in Adults with Obesity.” NEJM.
- NICE (2022). “Obesity: Identification, Assessment and Management.”
- UK Department of Health (2023). “Obesity: Healthcare System Review.”
- AHDB (2026). “Red Meat Market Outlook: Impact of Weight Loss Medications.”
- FDA (2023). “GLP-1 Receptor Agonists: Safety Communication on Suicidal Ideation.”