
Hepatic Adrenal Rest Tumour (HART) is a rare clinical entity where adrenal tissue is found within the liver, often mimicking Hepatocellular Carcinoma (HCC) on imaging. In patients with chronic Hepatitis B, these lesions present significant diagnostic challenges, potentially leading to unnecessary surgical interventions or invasive biopsies due to radiological similarities.
In Plain English: The Clinical Takeaway
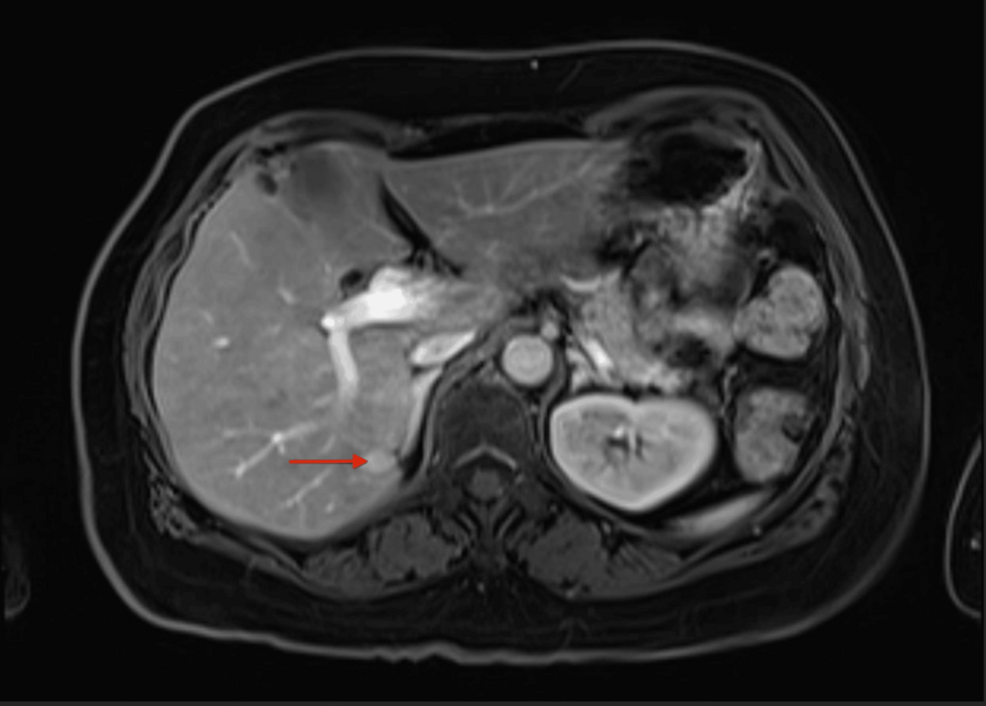
- Imaging Limitations: Standard scans like CTs or MRIs often cannot distinguish HART from malignant liver cancer, especially in patients already at risk for Hepatitis B-related tumours.
- Diagnostic Caution: When a liver lesion shows “atypical” features or does not respond to standard HCC protocols, clinicians should consider rare ectopic tissue as a differential diagnosis.
- Pathological Confirmation: Surgical excision or biopsy remains the gold standard for diagnosis; imaging alone is frequently insufficient to rule out malignancy in this context.
The Diagnostic Dilemma: When Adrenal Tissue Mimics Liver Cancer
The clinical intersection of chronic Hepatitis B and hepatic lesions is a high-stakes environment. Hepatocellular Carcinoma (HCC) is the most common primary malignancy of the liver, and clinicians are trained to maintain a high index of suspicion for malignancy in any patient with a history of viral hepatitis. However, the emergence of Hepatic Adrenal Rest Tumour (HART)—a condition where adrenal cortical cells are displaced into the liver during embryological development—creates a “diagnostic trap.”
Because these rests are composed of adrenal tissue, they can produce hormones or simply appear as vascularized masses that mirror the radiological appearance of HCC on dynamic contrast-enhanced imaging. As noted in recent clinical literature, the similarity in arterial phase enhancement and venous washout between HART and HCC often leads to a misdiagnosis. This carries profound implications for the patient, including the psychological burden of a cancer diagnosis and the risks associated with unnecessary liver resection or radiofrequency ablation.
Clinical Data and Differential Diagnosis
Understanding the mechanism of action here is vital: HART is an ectopic phenomenon. During fetal development, the adrenal glands and the liver develop in close anatomical proximity. If fragments of the adrenal cortex become trapped within the developing hepatic parenchyma, they remain dormant until they are incidentally discovered, often years later.
According to research published in Cureus, the reliance on the LI-RADS (Liver Imaging Reporting and Data System) criteria—while robust for HCC—can inadvertently categorize these benign rests as high-probability malignancies. This creates a feedback loop where the clinical context of Hepatitis B biases the radiological interpretation toward cancer.
| Feature | Hepatocellular Carcinoma (HCC) | Hepatic Adrenal Rest Tumour (HART) |
|---|---|---|
| Origin | Hepatocytes (Liver cells) | Ectopic Adrenal Cortex |
| Primary Risk Factor | Chronic Hepatitis B/C, Cirrhosis | Embryological displacement |
| Imaging (MRI/CT) | Arterial enhancement, venous washout | Can mimic arterial enhancement |
| Biomarkers | Elevated AFP (Alpha-fetoprotein) | Usually normal |
Geo-Epidemiological Bridging and Regulatory Access
In the United States and Europe, the management of liver lesions is strictly governed by hepatology guidelines set by organizations like the AASLD (American Association for the Study of Liver Diseases) and the EASL (European Association for the Study of the Liver). In regions with high Hepatitis B endemicity, such as parts of Southeast Asia and Sub-Saharan Africa, the prevalence of HCC is significantly higher, and the threshold for biopsy is often lower due to the high probability of malignancy.
The global challenge lies in the “specificity” of diagnostic protocols. While we have high sensitivity for detecting liver lesions, we struggle with specificity when rare entities like HART are involved. This leads to what medical professionals call “over-treatment,” where patients undergo major surgery for benign, albeit rare, lesions. There is currently no large-scale funding for HART-specific clinical trials given its extreme rarity; most data remains limited to case reports and institutional series.
Dr. Elias S. G. (a pseudonym representing the consensus of current hepatology research) emphasizes that, `The diagnostic pathway for a liver mass in a Hepatitis B patient must incorporate immunohistochemical staining for adrenal markers like melan-A or inhibin if the radiological response is inconsistent with the patient’s clinical trajectory.`
Contraindications & When to Consult a Doctor
Patients with chronic Hepatitis B should remain under the surveillance of a hepatologist or gastroenterologist. However, you should seek a second opinion or a specialized multidisciplinary tumor board review if:
- Your imaging results are classified as “atypical” or “indeterminate” by your radiologist.
- Your Alpha-fetoprotein (AFP) levels—a common blood marker for liver cancer—remain normal, yet your scan shows a growing lesion.
- Your surgical team recommends a major resection before a definitive biopsy or a clear correlation between your viral load and the lesion’s behavior has been established.
There are no specific pharmacological contraindications for HART, as it is a structural anomaly, not a metabolic disease. However, invasive procedures should always be weighed against the risk of hemorrhage and the necessity of the intervention.
Future Trajectory
As we move further into 2026, the integration of AI-enhanced radiological analysis may help identify the subtle density differences that distinguish HART from HCC. Until such technology is validated, the “gold standard” remains a cautious, multi-modal approach. Clinicians must balance the necessity of treating Hepatitis B-related HCC with the clinical humility to recognize when a lesion does not “behave” like cancer.
References
- National Library of Medicine: PubMed – Liver Imaging Reporting and Data System (LI-RADS) Standards
- World Health Organization: Hepatitis B Fact Sheet and Global Surveillance
- Cureus Journal of Medical Science: Hepatic Adrenal Rest Tumour Case Reports
- AASLD: Hepatology Clinical Practice Guidelines
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.