
Heart failure is a chronic condition where the heart cannot pump sufficient blood to meet the body’s metabolic needs. Identified by shortness of breath, extreme fatigue, and edema (swelling), it requires early detection and Guideline-Directed Medical Therapy (GDMT) to mitigate its high mortality rate and improve long-term survival.
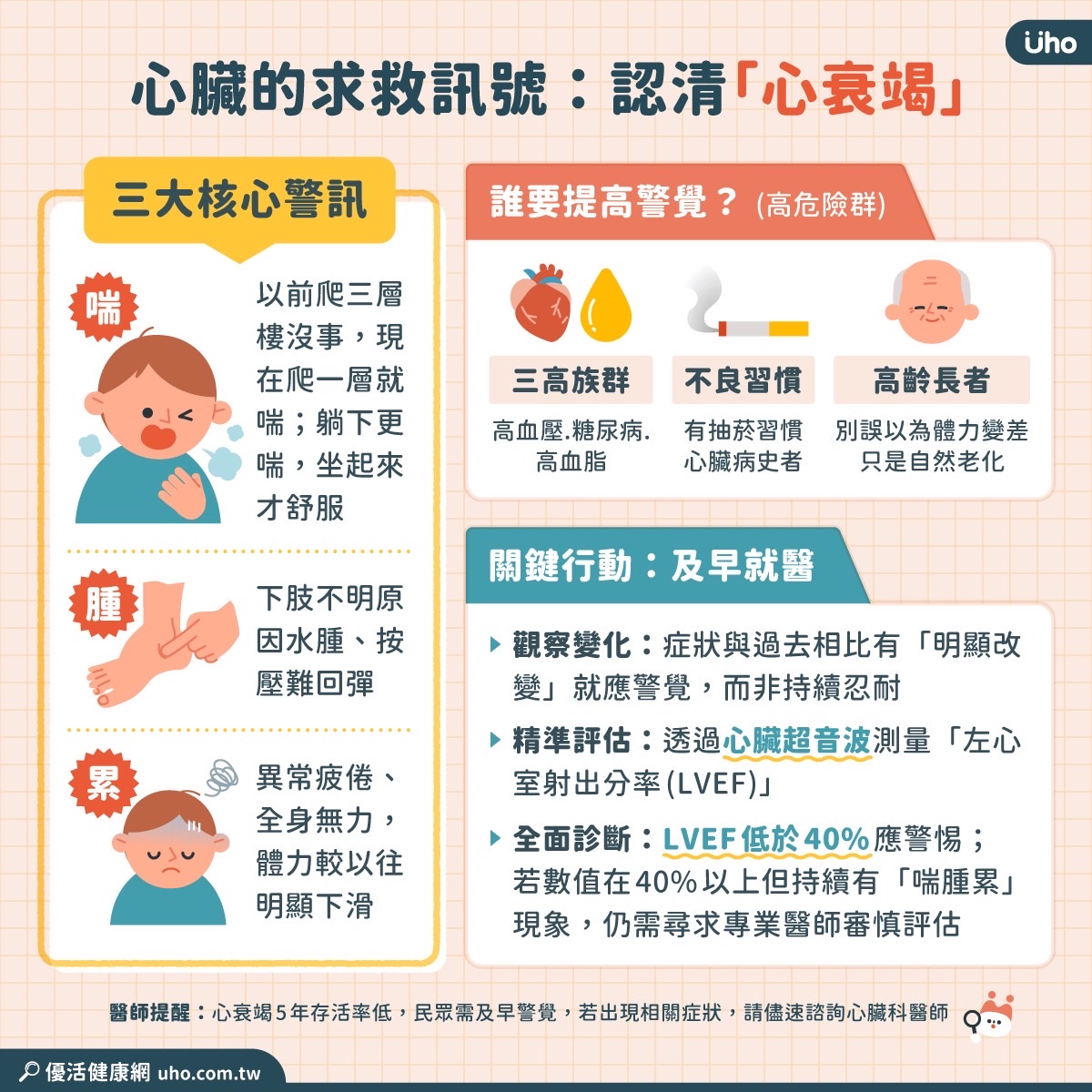
The clinical reality of heart failure (HF) is often misunderstood by the public as a sudden “stopping” of the heart. In truth, We see a progressive systemic decline. When the myocardium—the muscular tissue of the heart—weakens or stiffens, the body enters a state of hemodynamic instability. In other words the pressure and flow of blood are compromised, leading to a dangerous backlog of fluid in the lungs and extremities. For many patients, the window between the first sign of fatigue and a critical cardiac event is alarmingly narrow, making the “triad” of symptoms—breathlessness, exhaustion, and swelling—critical red flags that demand immediate clinical investigation.
In Plain English: The Clinical Takeaway
- Fluid Backup: When your heart fails as a pump, fluid leaks into your lungs (causing shortness of breath) and your ankles/legs (causing swelling).
- The “Silent” Decline: Fatigue is often dismissed as “aging,” but in HF, it is actually your muscles and organs starving for oxygenated blood.
- Manageable, Not Curable: While heart failure is chronic, modern medications can significantly extend life and improve quality of life if started early.
The Hemodynamic Cascade: Why Your Body Swells and Gasps for Air
To understand heart failure, one must understand the mechanism of action—the specific biological process—of the Renin-Angiotensin-Aldosterone System (RAAS). When the heart’s output drops, the kidneys perceive a lack of blood flow and trigger the RAAS to retain sodium and water to increase blood volume. While Here’s a survival mechanism for dehydration, in a failing heart, it is catastrophic.

This excess fluid increases the preload (the volume of blood returning to the heart), which the weakened ventricle cannot handle. The fluid then backs up into the pulmonary veins, leaking into the alveoli (air sacs) of the lungs. This is known as pulmonary edema, which manifests clinically as dyspnea—the medical term for shortness of breath—particularly when lying flat (orthopnea). Simultaneously, gravity pulls this excess fluid toward the lower extremities, resulting in peripheral edema, or visible swelling in the ankles and legs.
HFrEF vs. HFpEF: Understanding the Two Faces of Heart Failure
Not all heart failure is the same. Clinicians categorize the condition based on the Left Ventricular Ejection Fraction (LVEF), which is the percentage of blood pumped out of the left ventricle with each contraction. The distinction is critical because the treatment pathways differ significantly.

HFrEF (Heart Failure with reduced Ejection Fraction) occurs when the heart muscle becomes thin and weak, unable to contract effectively. Conversely, HFpEF (Heart Failure with preserved Ejection Fraction) occurs when the heart muscle becomes too stiff to fill properly, even though the pumping strength remains technically “normal.” HFpEF is increasingly common in aging populations, particularly among women and those with hypertension or diabetes.
| Feature | HFrEF (Reduced EF) | HFpEF (Preserved EF) |
|---|---|---|
| Ejection Fraction | < 40% | > 50% |
| Primary Issue | Systolic Dysfunction (Pumping) | Diastolic Dysfunction (Filling) |
| Common Cause | Myocardial Infarction (Heart Attack) | Hypertension, Obesity, Aging |
| Key Treatment | Beta-Blockers, ACEi/ARNI, SGLT2i | SGLT2i, Diuretics, Comorbidity Mgmt |
The Global Standard of Care and the “Fourth Pillar” of Therapy
The management of heart failure has evolved rapidly. We now utilize Guideline-Directed Medical Therapy (GDMT), a rigorous protocol of medications proven in double-blind placebo-controlled trials—studies where neither the patient nor the doctor knows who is receiving the treatment—to reduce mortality.
The current gold standard involves four “pillars” of therapy: Beta-blockers to reduce heart strain, ACE inhibitors or ARNIs to relax blood vessels, Mineralocorticoid Receptor Antagonists (MRAs) to prevent scarring, and the newest addition, SGLT2 inhibitors. Originally developed for diabetes, SGLT2 inhibitors have shown a remarkable ability to reduce HF hospitalizations regardless of whether the patient has diabetes. These findings, reinforced in recent updates to the American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines, have shifted the prognosis for millions.
“The integration of SGLT2 inhibitors into the standard of care represents one of the most significant shifts in heart failure management in a decade, providing a potent tool for reducing the risk of cardiovascular death across the entire spectrum of ejection fractions.” — Verified consensus from the Heart Failure Association of the ESC.
Regional Disparities and Geo-Epidemiological Impact
While the clinical guidelines are global, access varies. In East Asian healthcare systems, such as those in Taiwan and Japan, there is a higher prevalence of HFpEF linked to an aging demographic. However, the adoption of the “four pillars” of GDMT can be slower due to differing reimbursement policies for newer drugs like ARNIs (Angiotensin Receptor-Neprilysin Inhibitors). In contrast, the NHS in the UK and the FDA-regulated system in the US have integrated these drugs more rapidly into primary care, though socioeconomic barriers still hinder equitable access to these life-saving therapies.
Most of the pivotal trials for these medications were funded by pharmaceutical entities (such as AstraZeneca and Novartis), but the results have been independently verified by the Lancet and JAMA, ensuring that the clinical recommendations are based on data rather than corporate bias.
Contraindications & When to Consult a Doctor
While GDMT is life-saving, it is not universal. Certain medications have strict contraindications—conditions under which a drug must not be used. For example, ACE inhibitors are contraindicated in patients with a history of angioedema (severe swelling of the deep layers of the skin). Beta-blockers must be used with extreme caution in patients with severe asthma or certain bradycardias (abnormally slow heart rates).
Seek immediate emergency medical intervention if you experience:
- Acute Pulmonary Edema: Sudden, severe shortness of breath that worsens when lying flat, often accompanied by a cough producing frothy, pink-tinged sputum.
- Syncope: Fainting or sudden loss of consciousness due to inadequate cerebral perfusion.
- Rapid Weight Gain: An increase of more than 2-3 kg (approx. 5 lbs) within 2-3 days, indicating rapid fluid accumulation.
For those experiencing mild fatigue or intermittent swelling, a consultation with a cardiologist for an echocardiogram (an ultrasound of the heart) is the essential first step in preventing the progression toward end-stage heart failure.
References
- American Heart Association (AHA) – Heart Failure Guidelines 2024/2025.
- European Society of Cardiology (ESC) – Guidelines for the diagnosis and treatment of acute and chronic heart failure.
- The Lancet – Longitudinal studies on SGLT2 inhibitors and cardiovascular outcomes.
- World Health Organization (WHO) – Global Report on Cardiovascular Diseases.
- PubMed – Comparative analysis of HFrEF vs HFpEF pathophysiology.