
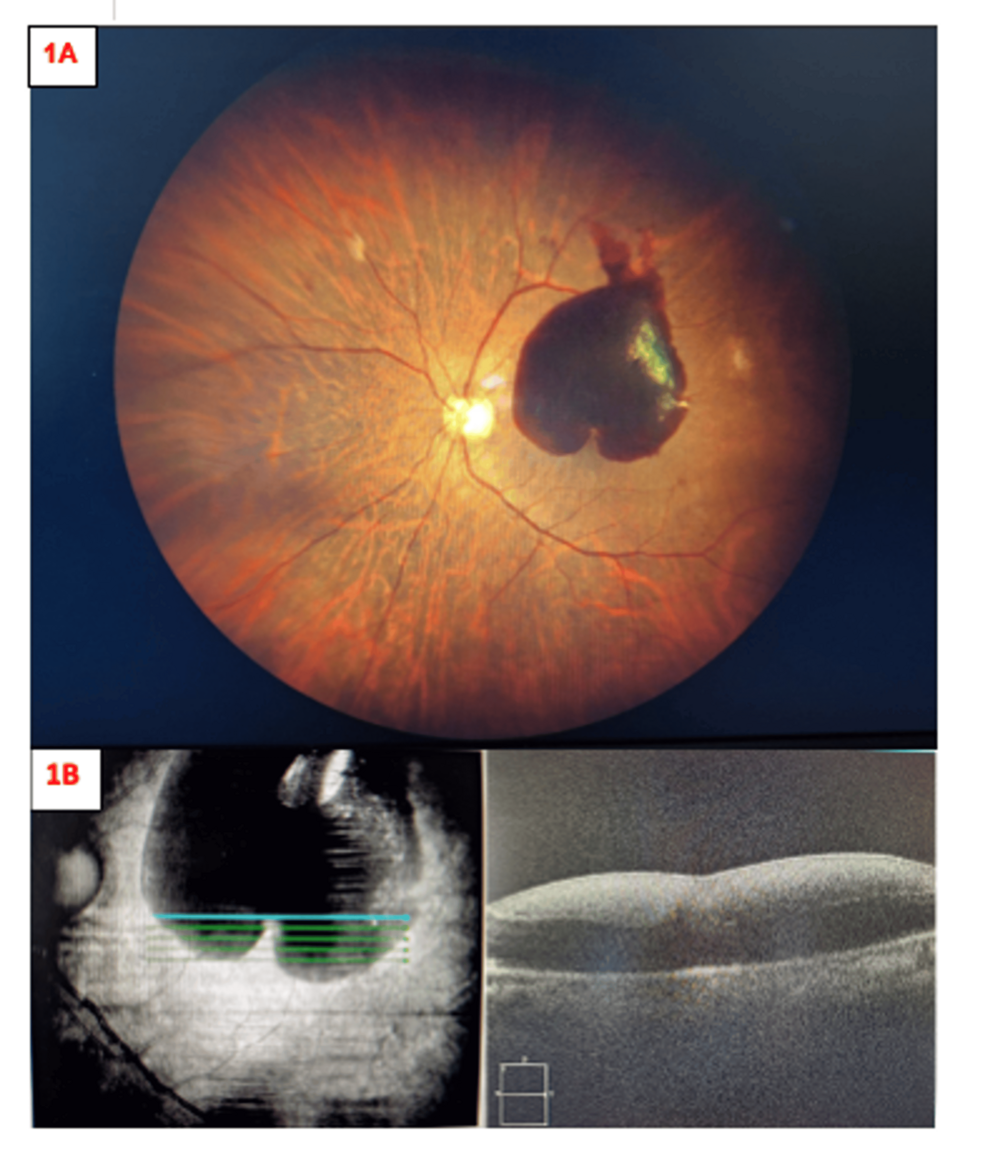
A heart-shaped subhyaloid haemorrhage—a localized pooling of blood between the retina and the vitreous humor—is a rare, vision-threatening complication of Valsalva retinopathy. Recent clinical documentation confirms that delayed, minimally invasive interventions, such as Nd:YAG laser hyaloidotomy, can successfully restore visual acuity even when initial presentation is significantly delayed.
In Plain English: The Clinical Takeaway
- Valsalva Retinopathy: This occurs when a sudden increase in internal chest pressure (like heavy lifting or coughing) causes small blood vessels in the eye to rupture.
- The “Heart” Shape: The blood pools beneath the hyaloid membrane (a thin layer covering the retina); its shape is determined by the pressure of the surrounding eye structures.
- Minimally Invasive Success: Even if the blood does not clear on its own, a laser procedure can safely drain the blood, often preventing the need for complex surgery.
Understanding the Pathophysiology of Valsalva Retinopathy
Valsalva retinopathy is a specific clinical entity precipitated by a sudden elevation in intra-thoracic or intra-abdominal pressure. This pressure surge is transmitted to the venous system of the eye, causing the delicate capillaries of the macula—the part of the retina responsible for sharp, central vision—to rupture. The resulting subhyaloid haemorrhage often presents as a distinct, gravity-dependent, heart-shaped or round lesion.
The “heart” morphology is a result of the unique anatomical attachment of the posterior hyaloid face to the retina. When blood accumulates, the physical constraints of this membrane dictate the shape of the clot. Clinically, this manifests as a sudden, painless scotoma, or a “blind spot,” in the patient’s visual field. According to research published in Cureus, while some cases resolve spontaneously, persistent haemorrhages can lead to toxic damage to the photoreceptors due to the prolonged presence of hemoglobin and iron-rich blood products.
Clinical Evolution and Minimally Invasive Intervention
The management of subhyaloid haemorrhage has shifted from invasive vitrectomy—a surgery to remove the vitreous gel—to less intrusive, office-based procedures. The use of the Neodymium-doped Yttrium Aluminium Garnet (Nd:YAG) laser has become a primary tool for “hyaloidotomy.” This mechanism of action involves focusing a high-energy laser pulse on the hyaloid membrane to create a small aperture, allowing the trapped blood to drain into the vitreous cavity, where it is more easily resorbed by the eye’s natural drainage system.
The recent case study highlights that even in delayed presentations, where the blood has begun to coagulate, this technique remains viable. By performing a laser hyaloidotomy, clinicians can bypass the risks associated with traditional intraocular surgery, such as infection (endophthalmitis) or cataract formation. Dr. David Pelayes, an expert in retinal imaging and pathology, has frequently noted in peer-reviewed literature that early identification is paramount, though modern laser techniques extend the therapeutic window for successful intervention.
Data Summary: Comparative Management Strategies
| Method | Invasiveness | Recovery Time | Primary Risk |
|---|---|---|---|
| Observation | None | Weeks to Months | Retinal toxicity/fibrosis |
| Nd:YAG Laser | Low (Office-based) | Days | Retinal detachment (rare) |
| Pars Plana Vitrectomy | High (Surgical) | Weeks | Cataract/Infection |
Geo-Epidemiological Context and Patient Access
The accessibility of these treatments varies by region. In the United Kingdom, the National Health Service (NHS) provides structured pathways for retinal emergencies, though access to sub-specialized laser suites may be centralized in tertiary eye hospitals. In the United States, patients covered by private insurance or Medicare typically have access to these procedures through retina specialists, provided the diagnosis is confirmed early via Optical Coherence Tomography (OCT).
Funding for the underlying research in this field is typically provided by institutional grants or academic departments, such as those associated with the National Eye Institute (NEI) in the U.S. or similar bodies within the European Medicines Agency (EMA) jurisdiction. Transparency in these studies is critical, as the choice between conservative observation and surgical intervention often hinges on the surgeon’s access to advanced imaging technology.
Contraindications & When to Consult a Doctor
Not every subhyaloid haemorrhage is a candidate for laser hyaloidotomy. Contraindications include the presence of a retinal detachment, uncontrolled proliferative diabetic retinopathy, or an inability of the patient to maintain the necessary head position during the laser procedure. Furthermore, if the haemorrhage is associated with underlying systemic clotting disorders, the primary cause must be managed before ocular intervention.
Patients should seek urgent ophthalmic consultation if they experience:
- Sudden, painless loss of vision in one eye.
- The appearance of a dark, stationary “curtain” or “spot” in their visual field.
- Visual symptoms following a strenuous physical event, such as heavy weightlifting or intense straining.
As of this week, clinical consensus remains that while Valsalva retinopathy is often self-limiting, the “heart-shaped” presentation warrants immediate imaging via OCT to assess the thickness of the blood layer and the integrity of the underlying retinal layers. Early, objective diagnostic assessment is the most effective defense against permanent vision loss.
References
- American Academy of Ophthalmology (AAO). “Retinal Vein Occlusions and Hemorrhagic Disorders.” aao.org
- National Eye Institute (NEI). “Types of Retinal Diseases and Management.” nei.nih.gov
- PubMed Central. “Valsalva Retinopathy: Mechanisms and Laser Hyaloidotomy Outcomes.” ncbi.nlm.nih.gov
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.