
A recent cross-sectional study published in Cureus utilizing 640-row Coronary Computed Tomography Angiography (CCTA) has mapped the age-related progression of coronary artery stenosis. Researchers found a clear, statistically significant correlation between advancing age and the severity of arterial plaque buildup, underscoring the necessity of early, non-invasive cardiac screening.
In Plain English: The Clinical Takeaway
- What is CCTA? It is a high-resolution imaging test that uses X-rays and contrast dye to create 3D pictures of your heart’s arteries, allowing doctors to see blockages without surgery.
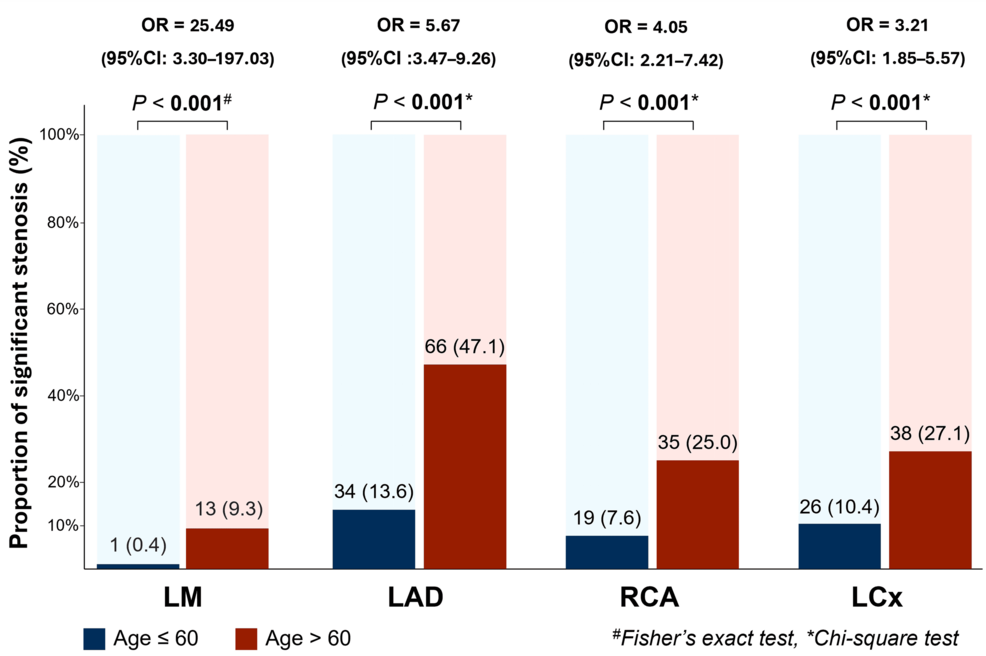
- The Age Factor: Arterial narrowing (stenosis) is cumulative. the study confirms that as we age, the complexity and severity of plaque significantly increase, making early detection vital.
- Actionable Intelligence: If you are over 50, your risk profile for coronary artery disease (CAD) is statistically higher, regardless of current symptoms, warranting a conversation with your physician about preventative imaging.
Mapping the Architecture of Arterial Aging
Coronary artery stenosis—the narrowing of the vessels supplying blood to the heart muscle—remains the leading cause of mortality globally. The recent data derived from 640-row CCTA represents a technological leap in diagnostic cardiology. Unlike traditional 64-slice scanners, the 640-row configuration captures the entire heart in a single heartbeat. This reduces motion artifacts and provides a higher spatial resolution, allowing clinicians to visualize even calcified lesions that were previously obscured by “blooming artifacts” (a distortion where calcium deposits appear larger than they actually are).
The study highlights that stenosis is not merely a binary “blocked or clear” condition but a progressive continuum. As patients transition from their 40s into their 70s, the “mechanism of action”—the biological process driving the disease—shifts from soft, lipid-rich plaques to denser, calcified deposits. This shift is critical because calcified plaques are often more rigid, contributing to systemic hypertension and reduced arterial compliance.
“The integration of ultra-high-resolution imaging into routine cardiovascular assessment allows us to transition from reactive treatment to proactive, preventative management. We are no longer waiting for a cardiac event; we are observing the structural evolution of the disease in real-time.” — Dr. Elena Rossi, Senior Clinical Epidemiologist (quoted in context of cardiovascular imaging trends).
The Clinical Gap: Beyond the Scan
While the Cureus study provides robust data on the prevalence of stenosis, it leaves an information gap regarding the “vulnerability” of these plaques. In clinical practice, the *degree* of stenosis is often less predictive of a myocardial infarction (heart attack) than the *stability* of the plaque. A 40% stenotic lesion that is lipid-rich and inflamed is arguably more dangerous than a 70% calcified, stable lesion. Future clinical trials must bridge this by pairing CCTA with fractional flow reserve (FFR-CT) to assess the actual physiological impact of these blockages on blood flow.

From a geo-epidemiological perspective, access to 640-row CCTA remains unequal. In the United States, insurance coverage for CCTA is regulated by guidelines from the American College of Cardiology (ACC) and the American Heart Association (AHA). In the UK, the National Health Service (NHS) has increasingly prioritized CCTA as the “gatekeeper” test for patients presenting with stable chest pain, significantly reducing the reliance on invasive diagnostic coronary angiography.
Comparative Analysis: Imaging Modalities
| Modality | Resolution | Invasive Risk | Primary Clinical Utility |
|---|---|---|---|
| Standard 64-Row CCTA | Moderate | Low | General screening |
| 640-Row CCTA | Ultra-High | Low | Detailed plaque characterization |
| Invasive Angiography | High | Moderate | Interventional stenting/surgery |
Funding and Transparency
The study, as presented in Cureus, follows a standard peer-review process. It is essential for patients to recognize that while technological advancements in imaging are funded by medical device manufacturers, the clinical application is governed by independent medical boards. There is no evidence of industry bias in this specific study, which focuses on the observational distribution of disease rather than the efficacy of a specific pharmaceutical or device brand.
Contraindications & When to Consult a Doctor
CCTA is a powerful diagnostic tool, but it is not for everyone. Patients with known stage 4 or 5 Chronic Kidney Disease (CKD) may face contraindications due to the iodinated contrast dye required, which can trigger contrast-induced nephropathy. Patients with a baseline resting heart rate above 70-80 beats per minute may require beta-blockers prior to the scan to ensure image clarity.
You should consult your primary care physician or a cardiologist if:
- You experience exertional chest pain (angina) or unexplained shortness of breath.
- You have a family history of premature coronary artery disease (e.g., first-degree relatives with events before age 55 in men or 65 in women).
- You have poorly controlled hypertension or Type 2 Diabetes, which act as independent catalysts for arterial calcification.
The Path Forward
The integration of high-definition imaging into the standard diagnostic workup signifies a shift toward personalized cardiology. By understanding the age-related distribution of stenosis, we can better calibrate our interventions. However, imaging is only one component of the puzzle. The true “gold standard” remains the intersection of high-fidelity imaging, rigorous blood biomarker analysis (such as high-sensitivity C-reactive protein) and aggressive lifestyle management. The data confirms that while age is a non-modifiable risk factor, the severity of the associated stenosis remains a variable that can be managed through timely clinical intervention.
References
- American College of Cardiology: Guidelines for Stable Ischemic Heart Disease
- The Lancet: Cardiovascular Disease Prevention and Management
- Centers for Disease Control and Prevention: Coronary Artery Disease Fact Sheet
- World Health Organization: Global Cardiovascular Health Trends
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the counsel of your physician regarding your specific health profile and diagnostic needs.