
Idiopathic Avascular Necrosis (AVN) of the femoral head, a condition characterized by the death of bone tissue due to interrupted blood supply, presents unique diagnostic challenges in older adults. Recent clinical evidence highlights the necessity of distinguishing this condition from common age-related orthopedic issues to prevent irreversible joint collapse and disability.
In Plain English: The Clinical Takeaway
- Bone Starvation: AVN occurs when the femoral head (the ball at the top of the thigh bone) loses its blood supply, causing the bone to die and eventually collapse.
- Diagnostic Complexity: Because hip pain in older adults is frequently attributed to osteoarthritis, AVN is often misdiagnosed or identified only at advanced stages.
- Proactive Imaging: If hip pain persists despite standard conservative treatment, clinicians should prioritize MRI scans, which are significantly more sensitive than X-rays for detecting early-stage bone necrosis.
The Mechanism of Ischemic Bone Death
Avascular necrosis, or osteonecrosis, follows a specific pathophysiological pathway: the disruption of microcirculation within the subchondral bone. While “idiopathic” implies the cause is unknown, medical literature increasingly links these events to subtle metabolic disturbances, coagulation abnormalities, or chronic micro-trauma. According to the Journal of the American Academy of Orthopaedic Surgeons, the femoral head is particularly vulnerable due to its precarious blood supply, primarily through the medial circumflex femoral artery.
In older adults, the clinical presentation is often confounded by comorbidities such as osteoporosis or rheumatoid arthritis. As noted in research published in Cureus, the absence of classic risk factors—such as long-term corticosteroid use or alcohol consumption—does not rule out AVN. When these factors are absent, the diagnosis requires a high index of clinical suspicion to differentiate the necrotic process from degenerative joint disease.
Diagnostic Imaging and Clinical Decision Making
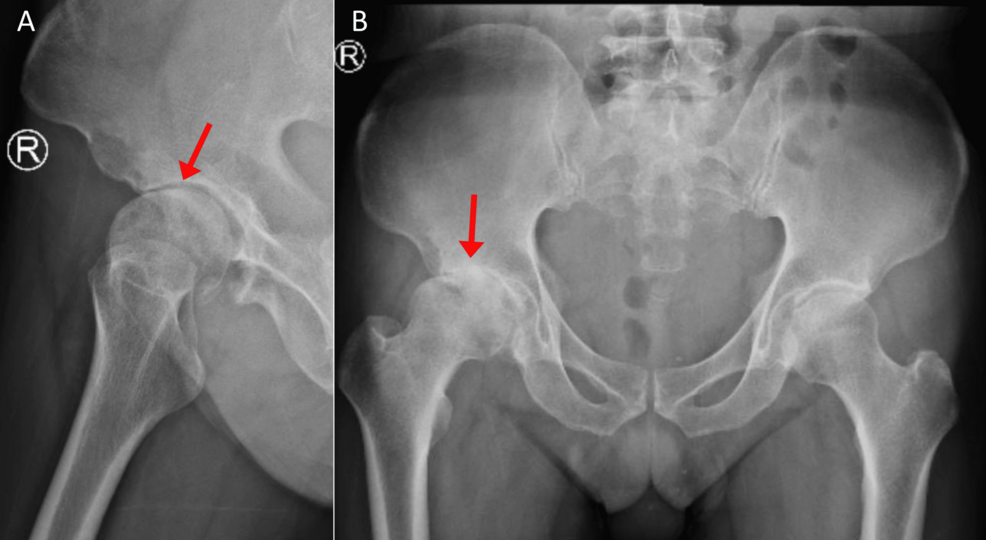
The standard of care for diagnosing hip pathology typically begins with plain radiographs. However, researchers emphasize that X-rays often appear normal in the early stages of AVN. Magnetic Resonance Imaging (MRI) remains the gold standard for early detection, offering the ability to visualize bone marrow edema—a swelling within the bone—before structural collapse occurs.
The following table summarizes the diagnostic hierarchy for suspected femoral head necrosis:
| Imaging Modality | Sensitivity for Early AVN | Clinical Utility |
|---|---|---|
| Plain Radiography (X-ray) | Low (< 50%) | Useful for identifying late-stage collapse. |
| Computed Tomography (CT) | Moderate | Superior for defining cortical bone integrity. |
| Magnetic Resonance Imaging (MRI) | High (> 95%) | Primary tool for early diagnosis and staging. |
Global Perspectives on Orthopedic Management
Healthcare systems, including the NHS in the United Kingdom and the FDA-regulated landscape in the United States, emphasize the importance of early intervention to preserve the natural hip joint. When AVN is caught in the pre-collapse stage, core decompression—a surgical procedure aimed at reducing pressure within the bone and stimulating new blood vessel growth—may be effective. Once the bone has collapsed, total hip arthroplasty (joint replacement) is frequently the only viable option to restore function.
Dr. Elena Rossi, an orthopedic researcher, notes: “The diagnostic delay in older populations is a critical barrier to joint preservation. We must move toward earlier MRI utilization in cases of unexplained, persistent hip pain.”
Contraindications & When to Consult a Doctor
Patients experiencing persistent, deep groin pain that worsens with weight-bearing activity should seek an orthopedic consultation. It is essential to note that anti-inflammatory medications may mask symptoms without addressing the underlying ischemic process.
Contraindications for Conservative Management:
- Radiographic Collapse: Once the femoral head has lost its spherical shape (as seen on imaging), physical therapy and conservative management are contraindicated, as they cannot reverse structural damage.
- Infection: Patients with suspected septic arthritis must be prioritized for urgent surgical evaluation, as AVN and infection require vastly different treatment protocols.
If you experience sudden inability to bear weight or night pain that disturbs sleep, consult a primary care physician or orthopedic specialist immediately to rule out osteonecrosis or other emergent vascular events.
Future Trajectory in Regenerative Orthopedics
The management of idiopathic AVN is shifting toward identifying occult risk factors earlier. Funding for research into the molecular triggers of bone ischemia remains a priority for organizations like the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). As diagnostic algorithms improve, the goal is to shift the treatment paradigm from salvage surgery to biological preservation.

References
- National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). Osteonecrosis: Diagnosis and Treatment.
- Journal of the American Academy of Orthopaedic Surgeons. Management of Avascular Necrosis of the Femoral Head.
- Cureus. Idiopathic Avascular Necrosis of the Femoral Head in an Older Adult: A Case Report.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions regarding a medical condition.