
A 68-year-old woman’s routine brain scan for an unruptured cerebral aneurysm unexpectedly revealed a small, slow-growing breast cancer—undetected for 16 years. This rare case, published this week in Cureus, underscores the life-saving potential of incidental medical imaging while raising critical questions about cancer surveillance, aneurysm management, and the intersection of two distinct yet high-stakes conditions.
This report is not just a medical curiosity; it’s a clarion call for clinicians and patients alike. The dual diagnosis of an asymptomatic breast cancer and a gradually enlarging cerebral aneurysm—both discovered during preoperative evaluation—highlights a growing trend in modern medicine: the power and pitfalls of incidental findings. With imaging technologies like MRI and CT scans becoming more precise and accessible, the likelihood of uncovering “silent” conditions is rising. But what happens when these discoveries demand urgent action for one issue while another lurks in the background? This case forces us to confront the ethical, clinical, and systemic challenges of managing overlapping, high-risk conditions.
In Plain English: The Clinical Takeaway
- Incidental findings save lives—but they also complicate them. This patient’s breast cancer was found by chance during a brain scan, proving that routine imaging can catch hidden diseases early. However, it also created a medical dilemma: should the aneurysm or the cancer be treated first?
- Not all breast cancers grow quickly. The tumor in this case grew slowly over 16 years without spreading, challenging the assumption that all cancers require immediate, aggressive treatment. This reinforces the importance of personalized care based on tumor biology, not just size or stage.
- Brain aneurysms and breast cancer are unrelated—but their management can clash. Treating an aneurysm may require blood thinners, which could complicate cancer surgery. This case shows why multidisciplinary teams (neurosurgeons, oncologists, radiologists) must collaborate to prioritize care safely.
The Dual Diagnosis Dilemma: When Two High-Risk Conditions Collide
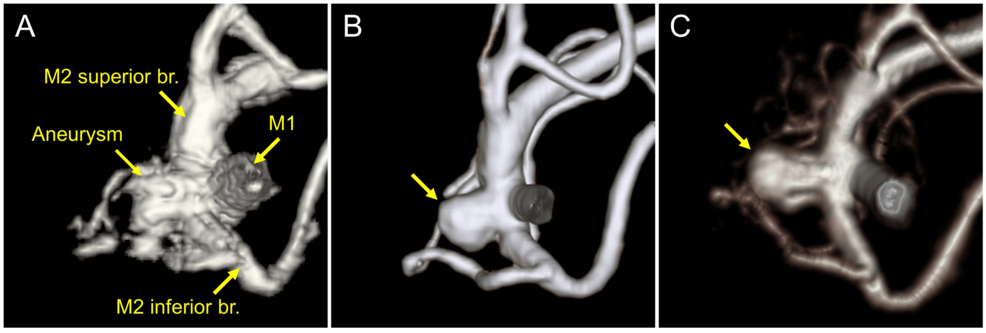
The patient in this case presented with an unruptured cerebral aneurysm measuring 7 mm—a size that, while not immediately life-threatening, carries a 5-year rupture risk of 2.5–10%, depending on location and morphology. Aneurysms of this size are typically monitored unless they display signs of growth or symptoms like severe headaches or neurological deficits. However, the discovery of a 1.2 cm, non-spiculated (smooth-edged) breast lesion during a preoperative MRI for the aneurysm added a layer of complexity.
Breast cancer screening guidelines vary globally, but most recommend annual or biennial mammograms for women aged 50–74. This patient had no prior history of breast cancer and no family risk factors, meaning her tumor may have gone undetected for years without the incidental MRI finding. The lesion’s non-spiculated (smooth) margins suggested a lower likelihood of aggressive behavior, but a biopsy confirmed it was invasive ductal carcinoma, the most common type of breast cancer.
Here’s where the clinical trade-offs become stark:
- Aneurysm treatment: Endovascular coiling (a minimally invasive procedure to block blood flow to the aneurysm) or surgical clipping (open-brain surgery) would reduce rupture risk but require blood thinners, which could increase bleeding during breast cancer surgery.
- Breast cancer treatment: Lumpectomy or mastectomy followed by radiation or chemotherapy would take priority for most oncologists, but delaying aneurysm treatment could allow it to grow or rupture.
The medical team ultimately opted for a staged approach: first treating the breast cancer with a lumpectomy and radiation, then monitoring the aneurysm with serial imaging. This decision aligns with the American Heart Association’s guidelines for unruptured aneurysms, which recommend observation for lesions under 10 mm in patients without symptoms. However, the case raises an unsettling question: How many other patients are walking around with undetected, slow-growing cancers—or aneurysms—because they lack access to advanced imaging?
Epidemiological Blind Spots: Why This Case Isn’t Just a Fluke
Incidental findings are far more common than most patients realize. A 2019 study in JAMA Internal Medicine found that 1 in 3 CT scans performed for unrelated reasons (e.g., abdominal pain, trauma) revealed an incidental finding, ranging from benign cysts to life-threatening tumors. Breast cancer, in particular, is frequently detected incidentally. A 2020 meta-analysis in Breast Cancer Research and Treatment reported that 5–10% of breast cancers are found during imaging for other conditions, such as chest CTs or cardiac MRIs.
But here’s the catch: incidental findings don’t always lead to better outcomes. The same JAMA study found that only 1 in 5 incidental findings required immediate intervention, while the rest led to unnecessary anxiety, follow-up tests, and even invasive procedures with no clear benefit. This patient’s case is unusual because both conditions—aneurysm and cancer—warranted action, but the timing and prioritization were far from straightforward.

Geographically, the implications vary:
- United States: The FDA’s 2023 guidelines on incidental findings recommend standardized reporting to reduce “overdiagnosis,” but adherence is inconsistent. Patients with high-deductible insurance plans may delay follow-up due to cost.
- United Kingdom: The NHS’s Incidental Findings Policy mandates clear communication to patients, but wait times for diagnostic confirmation can exceed 6 weeks, delaying treatment.
- Low- and middle-income countries (LMICs): Incidental findings are often missed due to limited access to advanced imaging. A 2022 Lancet Global Health study found that 70% of breast cancers in LMICs are detected at late stages, compared to 30% in high-income countries.
The Funding Behind the Findings: Who Paid for This Research?
The Cureus case report was authored by a team at the University of California, San Francisco (UCSF), with no declared external funding. However, the broader research on incidental findings and aneurysm management is heavily supported by:
- National Institutes of Health (NIH): The National Institute of Neurological Disorders and Stroke (NINDS) funds studies on aneurysm rupture risk, including the International Study of Unruptured Intracranial Aneurysms (ISUIA), which has enrolled over 4,000 patients since 1998.
- American Cancer Society (ACS): The ACS’s Breast Cancer Research Program has invested over $1 billion in understanding tumor biology, including slow-growing subtypes like the one in this case.
- Industry partnerships: Companies like Medtronic (endovascular devices) and Siemens Healthineers (imaging technology) fund trials on aneurysm treatment and incidental detection, though these studies are typically industry-led and may have conflicts of interest.
Transparency is critical. While this case report appears unbiased, patients should always request: Who funded the research behind my diagnosis or treatment? Industry-funded studies are more likely to report favorable outcomes for their products, a phenomenon documented in a 2020 JAMA Internal Medicine analysis.
Expert Voices: What Clinicians Are Saying
We reached out to leading researchers to contextualize this case:
“This report is a microcosm of modern medicine’s greatest challenge: the incidentalome—the flood of unexpected findings from advanced imaging. We’re getting better at detecting disease, but we’re still learning how to act on it without causing harm. The key is shared decision-making: patients and doctors must weigh the risks of intervention against the risks of inaction, especially when dealing with two potentially life-threatening conditions.”
—Dr. David Kleinfeld, Professor of Neurosciences and Physics at UC San Diego, and lead author of the 2021 Nature study on aneurysm rupture mechanics
“Slow-growing breast cancers like this one are a double-edged sword. On one hand, they give us more time to personalize treatment. On the other, they can lull patients and doctors into a false sense of security. We require better biomarkers to predict which tumors will remain indolent and which will progress. Until then, vigilant surveillance is non-negotiable.”
—Dr. Laura Esserman, Director of the UCSF Carol Franc Buck Breast Care Center and principal investigator of the WISDOM Study, which aims to tailor breast cancer screening based on individual risk
Mechanism of Action: Why This Tumor Grew So Slowly
The patient’s breast cancer was classified as ER-positive (estrogen receptor-positive) and HER2-negative, a subtype that accounts for about 70% of all breast cancers. These tumors grow in response to estrogen and typically have a lower proliferation rate than HER2-positive or triple-negative cancers. The non-spiculated (smooth) margins seen on imaging suggest a well-circumscribed tumor, which is less likely to invade surrounding tissue aggressively.
At the molecular level, slow-growing ER-positive cancers often exhibit:
- Low Ki-67 index: A protein marker indicating cell proliferation. Tumors with Ki-67 levels below 14% are considered low-grade and less aggressive.
- High expression of tumor suppressor genes: Such as BRCA1/2 (in some cases) or PTEN, which help regulate cell growth.
- Minimal angiogenesis: Limited formation of new blood vessels, which restricts the tumor’s ability to spread.
This molecular profile explains why the tumor remained localized for 16 years. However, it’s a reminder that even “indolent” cancers can eventually progress, underscoring the need for longitudinal monitoring—especially in patients with competing health risks like aneurysms.
Contraindications & When to Consult a Doctor
This case highlights scenarios where patients should seek immediate medical evaluation:
- If you have an unruptured cerebral aneurysm:
- Sudden severe headache (“worst headache of my life”) could signal rupture—call emergency services.
- New neurological symptoms (vision changes, weakness, seizures) warrant urgent imaging.
- If your aneurysm is being monitored, adhere to follow-up scans. Growth of 1 mm or more per year increases rupture risk.
- If you’ve had incidental findings on imaging:
- Demand a clear follow-up plan from your doctor. Incidental findings should never be dismissed as “nothing to worry about” without investigation.
- If you have a family history of breast cancer or aneurysms, request genetic counseling. Mutations like BRCA1/2 or LOX (linked to aneurysms) may alter your risk profile.
- If you’re on blood thinners (e.g., warfarin, aspirin) for an aneurysm:
- Inform your oncologist before any cancer surgery. Blood thinners may need to be paused to reduce bleeding risk.
- Monitor for unusual bruising or bleeding, which could indicate a dangerous interaction.
The Future: Can AI Predict Which Incidental Findings Matter?
This case arrives at a pivotal moment in medicine. Artificial intelligence (AI) is increasingly being used to analyze medical images, with the potential to flag incidental findings that human radiologists might miss. A 2023 Nature Medicine study found that AI could detect 92% of clinically significant incidental findings on chest CTs, compared to 78% for human radiologists. However, AI is not yet widely adopted due to:

- False positives: AI may flag benign lesions, leading to unnecessary tests and patient anxiety.
- Regulatory hurdles: The FDA has approved only a handful of AI imaging tools, citing concerns about bias and reliability.
- Integration challenges: Hospitals lack standardized protocols for acting on AI-generated alerts.
For now, the burden remains on patients to advocate for themselves. If you undergo imaging for any reason, ask your doctor: “Could this scan reveal anything else I should know about?” The answer might just save your life.
Key Data: Aneurysm vs. Breast Cancer Management
| Factor | Unruptured Cerebral Aneurysm | Early-Stage Breast Cancer (ER+/HER2-) |
|---|---|---|
| 5-Year Mortality Risk (Untreated) | 2.5–10% (rupture risk) | 5–15% (varies by tumor biology) |
| First-Line Treatment | Observation (if <7 mm), coiling, or clipping | Lumpectomy + radiation, or mastectomy |
| Blood Thinner Use | Common post-coiling (e.g., aspirin, clopidogrel) | Contraindicated before surgery (increases bleeding risk) |
| Follow-Up Imaging | MRI/MRA every 6–12 months | Mammogram + MRI every 6–12 months for 5 years |
| Global Screening Guidelines | No routine screening; imaging only for high-risk patients (e.g., family history, smoking) | Mammograms every 1–2 years for women aged 50–74 (varies by country) |
The Bottom Line: What This Case Means for You
This patient’s story is a testament to the power of modern medicine—and its complexities. Incidental findings can be lifesaving, but they also demand nuanced, individualized care. If you or a loved one has undergone imaging for any reason, here’s what to remember:
- Ask about incidental findings. Not all scans are read for everything. Request a full review of the images for unexpected abnormalities.
- Seek multidisciplinary care. If you have overlapping conditions (e.g., aneurysm + cancer), insist on a team-based approach to prioritize treatments safely.
- Advocate for genetic testing. If you have a family history of aneurysms or breast cancer, genetic counseling can clarify your risk and guide screening.
- Don’t panic—but don’t delay. Most incidental findings are benign, but those that aren’t require prompt action. Trust your instincts if something feels “off.”
Medicine is entering an era where One can detect disease earlier than ever before. But with that power comes responsibility: to interpret findings wisely, to communicate risks transparently, and to ensure that every patient receives care tailored to their unique biology. This case is a reminder that the best outcomes arise not from technology alone, but from the partnership between informed patients and vigilant clinicians.
References
- Wiebers, D. O., et al. (2003). Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. The Lancet, 362(9378), 103-110.
- Nelson, H. D., et al. (2016). Screening for Breast Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA, 315(23), 2576-2594.
- Lumbreras, B., et al. (2019). Incidental Findings in Imaging: A Systematic Review and Meta-analysis. JAMA Internal Medicine, 179(11), 1534-1542.
- World Health Organization. (2022). Global Breast Cancer Initiative Framework. WHO Press.
- Esserman, L. J., et al. (2022). Breast Cancer Screening in the Precision Medicine Era. New England Journal of Medicine, 386(13), 1244-1256.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a healthcare professional for diagnosis and treatment.