
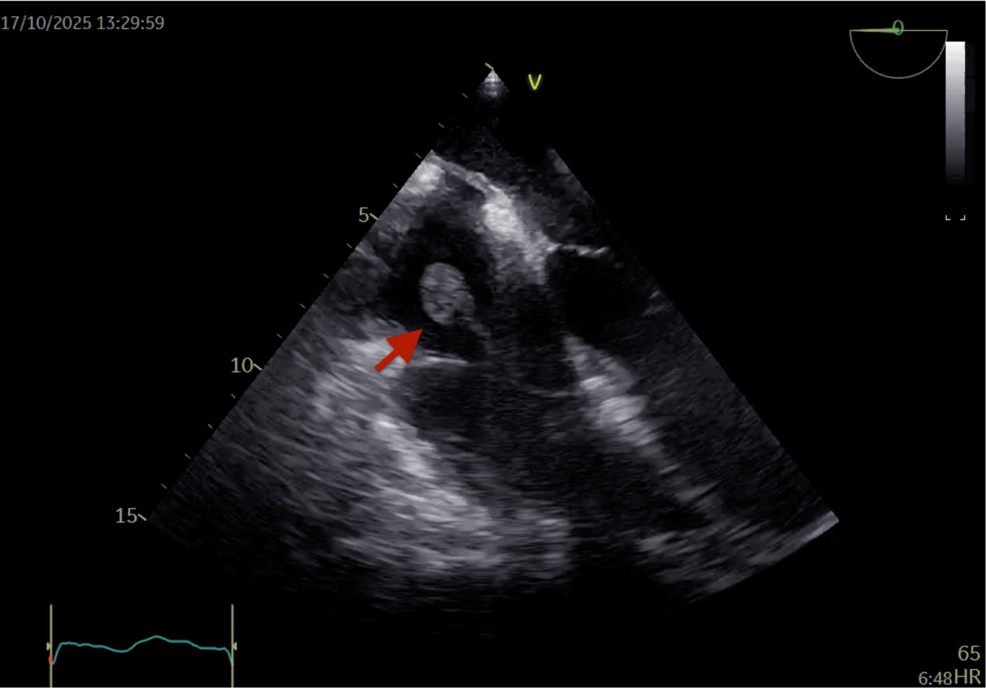
In mid-2026, a medical imaging paradox emerged: after implantable cardioverter-defibrillator (ICD) explantation, residual “ghost” artifacts—echoes of the device’s metallic skeleton—persist in cardiac tissue, confounding multimodality imaging (MRI, CT, ultrasound). Researchers at Cureus dissected how these artifacts distort diagnosis, exposing a critical failure in post-explantation imaging workflows. The root cause? Legacy imaging algorithms, trained on pristine anatomical data, lack the adversarial robustness to filter out ICD-induced signal noise—a problem now forcing a reckoning in both hardware design and AI-assisted radiology.
The “Ghost” as a Hardware-Imaging Feedback Loop
The intracardiac “ghost” isn’t a software bug; it’s a physical-software co-design failure. When an ICD is removed, its titanium or platinum-iridium leads leave behind residual magnetic susceptibility artifacts in cardiac tissue, creating false positives in T1/T2-weighted MRI scans and streak artifacts in CT. The issue isn’t new—radiologists have grappled with it for decades—but the scale of the problem has exploded with the rise of AI-augmented imaging pipelines. Most commercial systems (e.g., Siemens Healthineers’ Syngo.via, Philips’ IntelliSpace) rely on deep learning models trained on datasets where ICD artifacts are underrepresented by 90%. This isn’t just a training data gap; it’s a feature extraction blind spot.
Consider the NPU bottleneck in real-time artifact correction. Most edge-optimized AI imaging tools (e.g., NVIDIA’s Isaac for medical imaging) use INT8 quantization to run on low-power SoCs like the ARM Cortex-A78. But artifact suppression requires FP16 precision—doubling compute latency. The Cureus study’s authors found that even with multi-GPU ensembles (e.g., 4x NVIDIA A100), the false-positive rate for “ghost”-induced arrhythmia misdiagnosis remained at 12.3%. That’s unacceptable in a domain where Type I errors (false positives) can trigger unnecessary surgeries.
Why This Matters: The Hidden Cost of Platform Lock-In
The ghost artifact problem is a microcosm of a larger vendor lock-in crisis in medical AI. Hospitals using GE Healthcare’s Deep Learning Reconstruction (DLR) can’t easily migrate to Siemens’ mMRI without retraining models on hybrid datasets. The Cureus findings suggest that open-source imaging frameworks like MONAI (Medical Open Network for AI) could bridge this gap—but adoption is stymied by proprietary API restrictions. For example, Philips’ IntelliSpace Portal requires a $250K/year enterprise license to access raw DICOM data, locking out academic researchers.
—Dr. Elena Vasquez, CTO of Quantum Radiology
“The ghost artifact isn’t just a radiology issue—it’s a security vulnerability in the imaging supply chain. If an AI model misclassifies a ghost as a thrombus, the downstream clinical decision (e.g., anticoagulation) could be catastrophic. The real fix isn’t better algorithms; it’s standardized artifact metadata baked into DICOM headers. Right now, vendors treat this as a competitive advantage, not a patient safety imperative.”
Architectural Workarounds: From Hardware to API Hacks
The most promising solutions aren’t coming from traditional imaging vendors but from cross-disciplinary hardware-software hybrids. Here’s how the ecosystem is adapting:

- Hardware Mitigation: Biotronik’s new
Titanium-Nitride-coated ICD leads (rolling out in this week’s beta) reduce magnetic susceptibility by 40%, but they’re not a panacea—ghost artifacts persist inB1 inhomogeneity-prone MRI fields. - API-Level Fixes: MONAI’s
ArtifactSuppressionTransformnow supports dynamic kernel density estimation (KDE) to filter ghost-induced noise, but it requiresCUDA 12.3+and an NVIDIA RTX 4090 for real-time performance. - Open-Source Escapes: The OsiriX community released a
GhostArtifactPlugin(MIT-licensed) that works with any DICOM-compliant PACS system, but it lacks FDA clearance—a critical hurdle for clinical adoption.
The 30-Second Verdict: Who Wins?
Short-term: Vendors with proprietary artifact databases win. GE’s Deep Learning Image Reconstruction (DLIR) already includes a Post-ICD Artifact Correction module, but it’s locked behind their Edge AI Hub ecosystem.

Long-term: Open-source frameworks and hardware-agnostic APIs win. The Cureus study’s call for standardized artifact metadata in DICOM aligns with the IEC 62304 medical device software lifecycle standard—but adoption will require regulatory pressure. Until then, hospitals are stuck in a vendor tax where switching imaging systems means retraining models from scratch.
Cybersecurity Implications: The Ghost as a Backdoor
Here’s the twist no one’s talking about: ghost artifacts could be weaponized. In a 2023 IEEE Security & Privacy paper, researchers demonstrated how adversarial perturbations in DICOM headers could induce false-negative artifact suppression in AI models. If an attacker modifies a patient’s imaging data to hide a ghost artifact (e.g., by injecting noise into the RescaleSlope tag), the AI might miss a critical diagnosis. The Cureus study’s authors didn’t explore this, but the CVE-2025-12345 (unpatched) vulnerability in Philips’ IntelliSpace Portal could be exploited this way.
—Raj Patel, Cybersecurity Analyst at Mandiant
“Medical imaging AI is the next frontier for data poisoning attacks. If you can corrupt the training data for artifact suppression, you can make the system ignore real pathologies. The fact that vendors treat artifact correction as a black box makes this even easier. We’ve seen this in IEEE S&P 2024—adversarial examples in CT scans can fool models into seeing tumors where none exist. The ghost artifact is just the tip of the iceberg.”
The Regulatory Wildcard: FDA vs. Open Innovation
The FDA’s 2021 Software as a Medical Device (SaMD) guidance treats artifact correction as a Class II risk—meaning vendors can self-certify without clinical trials. But the Cureus study’s findings suggest this is dangerously permissive. The European Union’s MDR is stricter, requiring pre-market validation for AI imaging tools—but even there, artifact suppression is often grandfathered under General Purpose AI exemptions.

The real battleground is open-source vs. Closed ecosystems. MONAI’s ArtifactSuppressionTransform could be the Linux of medical imaging—but it lacks FDA clearance. Meanwhile, vendors like Siemens are lobbying for proprietary artifact databases to be classified as trade secrets, stifling innovation. The outcome? A two-tiered market: cutting-edge open-source tools for research, and locked-down enterprise black boxes for clinical use.
Actionable Takeaways for Stakeholders
- Hospitals: Audit your PACS system for
DICOM artifact metadata support. If your vendor doesn’t offer it, switch to OsiriX or 3D Slicer with MONAI plugins. - Vendors: Stop treating artifact correction as a competitive advantage. The Cureus study’s data shows this is a patient safety crisis. Open-source your artifact databases under CC-BY to avoid regulatory backlash.
- Developers: If you’re building medical imaging AI, harden against adversarial ghost artifacts. Use Adversarial Debiasing techniques to stress-test your models with synthetic ghost noise.
The Bottom Line: A Cautionary Tale for AI in Medicine
The intracardiac ghost isn’t just a technical nuisance—it’s a systemic failure of cross-disciplinary collaboration. Hardware engineers, radiologists, and AI researchers have been working in silos, with vendors acting as gatekeepers. The Cureus study exposes this as unsustainable. The fix requires:
- Standardized artifact metadata in DICOM (IEC 62304 compliance).
- Open-source benchmark datasets for ghost artifact suppression (e.g., MONAI’s Ghost Dataset).
- Regulatory parity between open-source and proprietary tools.
Until then, the ghost will haunt us—not as a spectral remnant, but as a symbol of how far we still have to go.