
Ketamine-induced cystitis is a debilitating inflammatory condition characterized by severe bladder wall thickening and capacity loss. Primarily affecting recreational users and some therapeutic patients, this “ketamine bladder” causes extreme urgency and pain, often necessitating aggressive urological intervention to prevent permanent renal failure or total bladder removal.
The rise of ketamine—both as a revolutionary treatment for treatment-resistant depression and as a widespread recreational drug—has created an unforeseen urological crisis. Even as the psychiatric benefits are documented, the systemic toxicity to the urinary tract is often overlooked until the damage is irreversible. For patients, this means a devastating paradox: a drug intended to save a mind may inadvertently destroy a vital organ.
In Plain English: The Clinical Takeaway
- Chemical Irritation: Ketamine breaks down into metabolites that act like “chemical sandpaper” on the bladder lining, causing chronic inflammation.
- Capacity Loss: The bladder shrinks (decreased capacity), which can lead to the need to urinate every 15 to 30 minutes.
- The Only Cure: Complete cessation of ketamine use is the only definitive way to halt the progression of the disease and allow the bladder to heal.
The Molecular Mechanism of Urothelial Destruction
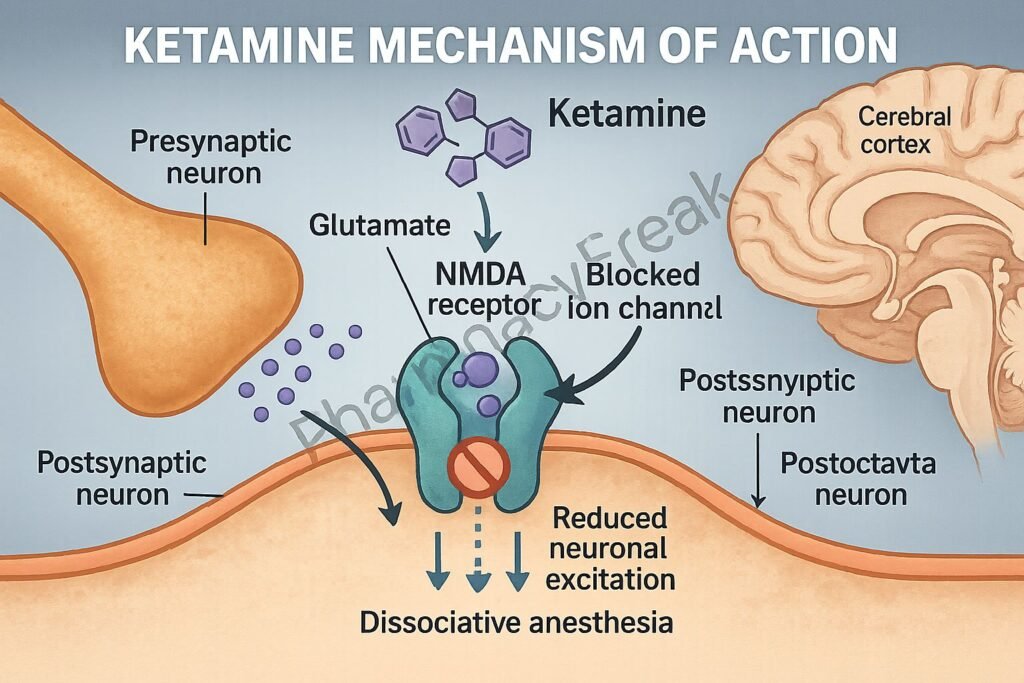
To understand why ketamine targets the bladder, we must examine its mechanism of action—the specific biochemical interaction through which a drug produces its effect. While ketamine is primarily known as an NMDA receptor antagonist in the brain, its metabolites, specifically norketamine, are excreted through the kidneys into the urine.
These metabolites act as direct irritants to the urothelium, the specialized layer of cells lining the bladder. This triggers a cascade of inflammatory responses, leading to the shedding of these cells and the exposure of the underlying basement membrane. Over time, the bladder undergoes fibrosis—the formation of excess fibrous connective tissue—which transforms a flexible, expandable organ into a rigid, shrunken sac.
This process is often categorized as a double-blind placebo-controlled variable in psychiatric studies, but in the real world, it manifests as “ketamine-induced cystitis.” The result is a profound decrease in bladder volume, often dropping from a healthy 400-500ml to as little as 20-50ml in severe cases.
“The severity of ketamine-induced cystitis is often underestimated until the patient presents with a bladder so small that the quality of life is effectively zero. We are seeing a shift from manageable inflammation to permanent structural failure.”
Global Epidemiological Trends and Regulatory Gaps
The prevalence of this condition varies significantly by region, reflecting different patterns of drug access and usage. In the United Kingdom, the National Health Service (NHS) has reported a surge in young adults presenting with “ketamine bladder,” leading to an increase in cystectomies (surgical removal of the bladder). In contrast, the United States has seen a rise in therapeutic use through FDA-approved esketamine (Spravato) and off-label intravenous infusions.
While therapeutic doses are significantly lower than recreational doses, the clinical community remains vigilant about long-term exposure. The FDA and the European Medicines Agency (EMA) have focused primarily on the psychiatric safety and dissociative effects of ketamine, but there is a growing demand for stricter urological monitoring protocols for patients on long-term ketamine therapy.
Most of the foundational research into this toxicity has been funded by academic institutions and public health grants, such as those from the National Institutes of Health (NIH), rather than pharmaceutical companies. This independence is crucial, as it ensures that the risks of bladder toxicity are reported without the bias of profit motives associated with the expanding psychedelic medicine market.
Clinical Comparison: Recreational vs. Therapeutic Impact
The risk profile of ketamine toxicity is heavily dose-dependent. The following table summarizes the typical clinical presentation across different usage patterns observed in recent urological cohorts.

| Metric | Recreational Use | Therapeutic Use (Clinically Supervised) |
|---|---|---|
| Typical Dosage | High/Frequent (Gram levels) | Low/Intermittent (Milligram levels) |
| Incidence of Cystitis | High (Common in chronic users) | Rare (Low-frequency risk) |
| Bladder Capacity | Severe Reduction (often <. 100ml) | Generally Maintained |
| Primary Symptom | Extreme Urgency/Hematuria | Mild Irritation (if any) |
| Recovery Potential | Variable (Depends on fibrosis) | High (due to lower cumulative dose) |
The Path to Recovery and Management
Management of ketamine-induced cystitis is primarily focused on abstinence. Once the drug is removed from the system, some patients experience a partial recovery of bladder capacity. However, for those who have reached the stage of severe fibrosis, the damage is permanent.
Medical interventions currently include the use of anti-inflammatory medications and, in extreme cases, the surgical implantation of an augmented bladder or a urinary diversion. Research published in PubMed suggests that early detection through cystoscopy—a procedure where a camera is inserted into the bladder—is critical for preventing total organ failure.
The intersection of neurology and urology is where the battle for the patient’s quality of life is fought. We must balance the efficacy of ketamine in treating suicidal ideation against the statistical probability of inducing a lifelong urological disability.
Contraindications & When to Consult a Doctor
Ketamine therapy is not suitable for everyone. Contraindications—conditions or factors that serve as a reason to withhold a certain medical treatment—include a history of severe interstitial cystitis, chronic kidney disease, or uncontrolled hypertension.
Patients should seek immediate urological consultation if they experience the following “red flag” symptoms:
- Hematuria: The presence of blood in the urine, which may indicate severe urothelial erosion.
- Frequency: A sudden, drastic increase in the need to urinate (e.g., every 15-30 minutes).
- Suprapubic Pain: Intense pressure or pain in the lower abdomen.
- Urgency: An uncontrollable, sudden urge to urinate that cannot be delayed.
Early intervention is the difference between a manageable condition and a life-altering surgery. If you are undergoing ketamine treatment for mental health, ensure your provider is coordinating care with a urologist to monitor bladder health.
As we move further into 2026, the medical community must move past the novelty of “psychedelic breakthroughs” and implement rigorous, long-term safety monitoring. Ketamine is a powerful tool, but like all potent medications, its utility is defined by the balance of its risks. The bladder should not be the price of mental wellness.