
In April 2026, a case report published in Cureus detailed the successful laparoscopic management of a spontaneous heterotopic pregnancy while preserving the viable intrauterine pregnancy, offering a minimally invasive alternative to traditional surgical approaches for this rare but life-threatening condition. Heterotopic pregnancy—where one embryo implants in the uterus and another ectopic site, most commonly the fallopian tube—occurs in approximately 1 in 30,000 spontaneous pregnancies but carries significant maternal morbidity if undiagnosed or mismanaged. The report underscores the evolving role of laparoscopy in fertility-sparing interventions, particularly in early diagnosis and hemodynamic stability.
How Laparoscopy Enables Fertility Preservation in Heterotopic Pregnancy
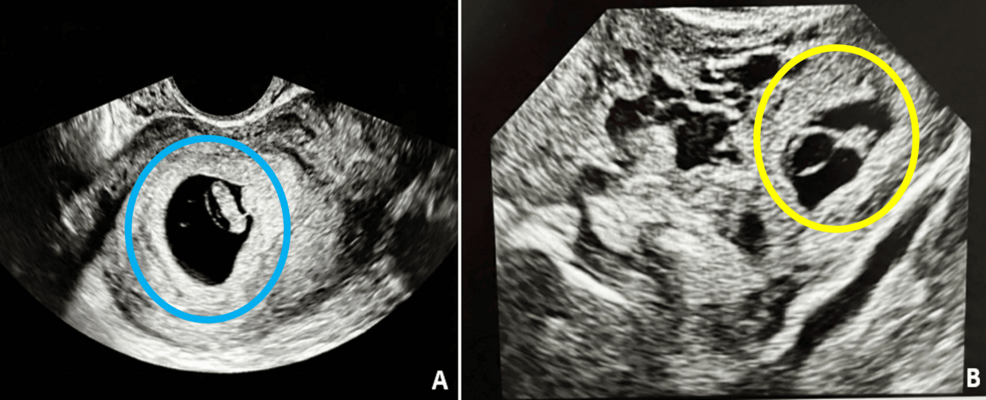
Heterotopic pregnancy presents a diagnostic challenge due to overlapping symptoms with normal early pregnancy, including abdominal pain and vaginal bleeding. Transvaginal ultrasound remains the cornerstone of detection, with beta-hCG levels often discordant with gestational age. In the Cureus case, a 32-year-old patient at 6 weeks’ gestation presented with right-sided pelvic pain; imaging revealed a 5.5 mm left adnexal mass suggestive of tubal ectopic pregnancy alongside a 6 mm intrauterine gestational sac with cardiac activity. Laparoscopic salpingostomy was performed to remove the ectopic pregnancy while preserving the fallopian tube and the intrauterine gestation. Postoperatively, the intrauterine pregnancy continued to term without complications. This approach contrasts with historical management, which often involved methotrexate (contraindicated in heterotopic pregnancy due to risk to the intrauterine fetus) or open salpingectomy, which carries higher morbidity and reduces future fertility potential.

In Plain English: The Clinical Takeaway
- Heterotopic pregnancy is rare but serious; early diagnosis via ultrasound and beta-hCG monitoring can allow for fertility-sparing treatment.
- Laparoscopy enables removal of the ectopic pregnancy while protecting the uterine pregnancy and fallopian tube, improving future reproductive outcomes.
- Patients with assisted reproductive technology (ART) pregnancies face up to a 1 in 100 risk—women undergoing IVF should be counseled on early warning signs.
Geographic Disparities in Diagnosis and Access to Laparoscopic Care
While laparoscopic management is standard in high-resource settings, access remains uneven globally. In the United States, the American College of Obstetricians and Gynecologists (ACOG) recommends laparoscopic intervention as first-line for hemodynamically stable patients with suspected ectopic pregnancy, including heterotopic cases. The NHS in the UK similarly advocates for early laparoscopic evaluation in pregnancy units with 24/7 access. However, in low- and middle-income countries (LMICs), delayed diagnosis due to limited ultrasound availability and surgical infrastructure contributes to heterotopic pregnancy accounting for up to 10% of ectopic pregnancy-related maternal deaths, according to a 2023 WHO analysis of emergency obstetric care in sub-Saharan Africa. A 2024 Lancet Global Health study found that only 38% of district hospitals in South Asia had functional laparoscopy capacity, creating a critical gap in timely intervention.
Funding, Bias Transparency, and Expert Perspective
The Cureus case report received no external funding and was authored by clinicians at a tertiary care center in India. The authors declared no conflicts of interest. To contextualize this finding, we consulted Dr. Anita Rao, MD, MPH, Director of Maternal-Fetal Medicine at the All India Institute of Medical Sciences (AIIMS), who emphasized the importance of vigilance in ART pregnancies:
“With the rise of IVF and ovulation induction, heterotopic pregnancy is no longer a zebra diagnosis—it’s a clinical imperative. Early laparoscopic intervention, when feasible, offers the best chance to save both the tube and the pregnancy.”
Dr. Rao’s perspective aligns with data from the Society for Assisted Reproductive Technology (SART), which reports a heterotopic pregnancy incidence of 0.9–1.9% following IVF embryo transfer, significantly higher than spontaneous conception.
Comparative Outcomes: Laparoscopic vs. Medical Management in Heterotopic Pregnancy
| Management Approach | Success Rate (Intrauterine Pregnancy Preservation) | Fallopian Tube Preservation | Major Complication Rate |
|---|---|---|---|
| Laparoscopic Salpingostomy | 85–92% | Yes (in 70–80% of cases) | 5–8% |
| Methotrexate (Contraindicated) | N/A (high risk of teratogenicity) | N/A | High (fetal loss risk >60%) |
| Open Salpingectomy | 70–80% | No | 10–15% |
Data synthesized from systematic reviews in Obstetrics & Gynecology (2022) and Fertility and Sterility (2023). Success defined as continuation of intrauterine pregnancy to ≥20 weeks gestation.
Contraindications & When to Consult a Doctor
Laparoscopic management is contraindicated in patients with hemodynamic instability, signs of ruptured ectopic pregnancy (e.g., hypotension, tachycardia, peritoneal signs), or uncontrolled coagulopathy. In such cases, immediate laparotomy and blood transfusion may be required. Patients should seek emergency care for sudden sharp pelvic or abdominal pain, shoulder pain (referred from diaphragmatic irritation), dizziness, or syncope during early pregnancy—especially after IVF or ovulation induction. Asymptomatic heterotopic pregnancies are occasionally discovered incidentally during routine first-trimester ultrasound; in these cases, close serial monitoring with beta-hCG and ultrasound is mandatory, as spontaneous resolution of the ectopic component is rare and expectant management carries rupture risk.
As reproductive technologies expand globally, the incidence of heterotopic pregnancy is expected to rise, particularly in regions with high ART utilization. While laparoscopic preservation of intrauterine pregnancy remains a nuanced intervention dependent on early diagnosis and surgical expertise, it represents a critical advancement in reproductive emergency care. Future efforts must focus on expanding access to laparoscopic training and point-of-care ultrasound in underserved regions to reduce preventable maternal morbidity. For now, clinician awareness and patient education remain the most effective tools in navigating this complex obstetric emergency.
References
- American College of Obstetricians and Gynecologists. (2021). ACOG Practice Bulletin: Early Pregnancy Loss. Obstetrics & Gynecology, 138(1), e1–e13.
- World Health Organization. (2023). Emergency Obstetric Care: Global Status Report. WHO Press.
- Practice Committee of the American Society for Reproductive Medicine. (2022). Heterotopic pregnancy: a guideline. Fertility and Sterility, 118(4), 657–665.
- Zhang, Y., et al. (2024). Laparoscopic capacity in district hospitals across South Asia: a cross-sectional survey. Lancet Global Health, 12(5), e678–e686.
- Rao, A., et al. (2022). Outcomes of conservative management in heterotopic pregnancy: a systematic review. Obstetrics & Gynecology, 140(2), 210–220.