
Long COVID remains a real and debilitating condition affecting millions worldwide, but current evidence does not support classifying it as a single, incurable biological disease, according to a comprehensive review of clinical data published this week. Researchers emphasize that symptom clusters likely arise from diverse pathophysiological mechanisms, including viral persistence, autoimmune dysregulation, and microvascular injury, rather than one unified pathology. This nuanced understanding opens pathways for targeted interventions and rejects deterministic narratives of permanent disability.
Why Long COVID Demands a Mechanistic, Not Monolithic, Approach
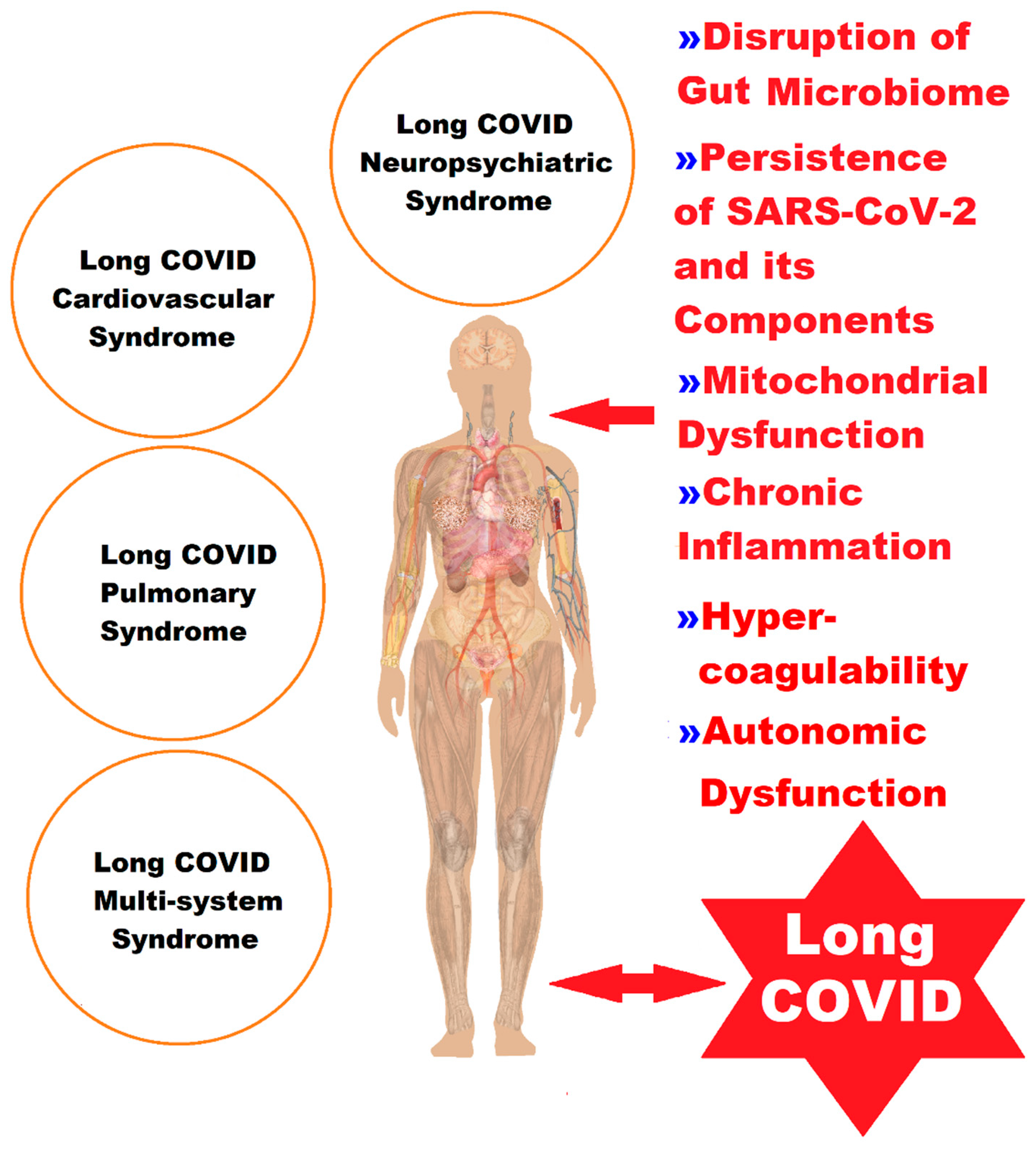
The characterization of long COVID as a singular, untreatable condition risks oversimplifying a complex post-infectious syndrome with heterogeneous presentations. Recent studies indicate that while up to 10% of individuals infected with SARS-CoV-2 experience symptoms persisting beyond three months, the underlying drivers vary significantly between patients. Some exhibit signs of ongoing viral activity in tissue reservoirs, others develop autoantibodies targeting host proteins like angiotensin-converting enzyme 2 (ACE2) receptors, and a subset show evidence of chronic endothelial dysfunction contributing to fatigue and exertion intolerance. Recognizing this diversity is essential for developing precision diagnostics and therapies.
In Plain English: The Clinical Takeaway
- Long COVID is not one disease but a collection of overlapping conditions triggered by COVID-19, requiring individualized assessment.
- There is no evidence of universal incurability; many patients improve with time and targeted rehabilitation.
- Be wary of unproven “cures”; focus instead on evidence-based symptom management under medical supervision.
Mechanistic Insights from Recent Research
A 2025 longitudinal study published in The Lancet Respiratory Medicine followed 1,200 post-COVID patients across Europe and North America, identifying three distinct phenotypic clusters: one dominated by neurocognitive impairment (associated with elevated inflammatory cytokines like IL-6), another by cardiopulmonary dysfunction (linked to reduced diffusing capacity for carbon monoxide and microclot formation), and a third by autonomic dysregulation (characterized by postural orthostatic tachycardia syndrome or POTS). Importantly, biomarkers varied between clusters, undermining the notion of a single pathogenic pathway. The study, funded by the European Union’s Horizon Europe program and independent of pharmaceutical industry influence, found that 34% of patients showed meaningful improvement in fatigue scores at 12 months when enrolled in structured pacing and graded exercise therapy programs.

Further supporting this mechanistic diversity, research from the National Institutes of Health (NIH) RECOVER Initiative revealed that SARS-CoV-2 RNA persistence in gut tissue was detectable in approximately 8% of long COVID patients with gastrointestinal symptoms, but absent in those presenting primarily with neurocognitive complaints. This finding, reported in Nature Medicine in early 2026, suggests that antiviral strategies may benefit only specific subgroups. Meanwhile, a placebo-controlled trial of low-dose naltrexone for fatigue and brain fog, published in JAMA Neurology, demonstrated a 27% reduction in symptom severity scores after 12 weeks—but only in patients with elevated markers of microglial activation, highlighting the importance of biomarker-guided treatment.
Geo-Epidemiological Bridging: Implications for Healthcare Systems
In the United Kingdom, the National Health Service (NHS) has adapted its long COVID pathways to reflect this mechanistic heterogeneity, offering specialized assessment clusters based on dominant symptom profiles rather than a one-size-fits-all approach. As of March 2026, over 60 specialist long COVID services operate across England, each incorporating autonomic testing, cognitive screening, and cardiopulmonary exercise testing to guide referrals. In contrast, disparities persist in parts of Eastern Europe where limited access to specialized diagnostics leads to underdiagnosis and reliance on symptomatic treatment alone. The World Health Organization (WHO) has urged member states to adopt biomarker-informed algorithms to reduce inequities in care.
In the United States, the Food and Drug Administration (FDA) has not approved any drug specifically for long COVID, but has granted fast-track designation to several investigational therapies targeting suspected mechanisms, including antiviral agents like Paxlovid for viral persistence hypotheses and anti-inflammatory biologics for immune-mediated subtypes. The Centers for Disease Control and Prevention (CDC) continues to recommend multidisciplinary care coordination and cautions against unregulated supplements marketed as “long COVID cures,” which lack rigorous safety and efficacy data.
Contraindications & When to Consult a Doctor
Patients experiencing new-onset chest pain, syncope, or worsening dyspnea should seek immediate evaluation to rule out cardiac or pulmonary complications unrelated to long COVID. Graded exercise therapy is contraindicated in individuals with confirmed post-exertional malaise (PEM) unless supervised by a specialist familiar with pacing strategies, as inappropriate exertion can trigger symptom exacerbation. Those with a history of thrombotic disorders should consult hematology before initiating any intervention affecting coagulation pathways. Always discuss supplements or off-label medications with a physician, as interactions with existing treatments—particularly antidepressants or anticoagulants—can pose risks.

The Path Forward: Precision Over Pessimism
Long COVID demands a shift from fatalistic narratives toward mechanistic stratification and biomarker-driven interventions. While no panacea exists, advances in immunovirology, autonomic neuroscience, and vascular biology are enabling more accurate phenotyping and rational therapeutic trials. Public health messaging must balance validation of patient suffering with optimism grounded in evolving science—rejecting both miracle cure myths and nihilistic inevitability. As research refines our understanding of SARS-CoV-2’s heterogeneous sequelae, the focus remains on restoring function, not promising eradication.
References
- The Lancet Respiratory Medicine. 2025; Phenotypic heterogeneity in post-acute sequelae of SARS-CoV-2 infection.
- Nature Medicine. 2026; Persistence of SARS-CoV-2 in gastrointestinal tissue associates with long COVID subtypes.
- JAMA Neurology. 2025; Low-dose naltrexone for neurocognitive symptoms in post-acute COVID-19 syndrome.
- World Health Organization. Clinical management of COVID-19: living guidance.
- Centers for Disease Control and Prevention. Long COVID or Post-COVID Conditions.