
A recent case report published in Cureus demonstrates that patients experiencing ADHD medication shortages can successfully transition from extended-release formulations to immediate-release (IR) dextroamphetamine without loss of symptom control. This finding offers a clinical pathway for maintaining therapeutic stability when preferred long-acting stimulants are unavailable due to supply chain disruptions.
In Plain English: The Clinical Takeaway
- Therapeutic Interchange: Patients forced to switch medications due to shortages can maintain efficacy by adjusting the dosing frequency of immediate-release stimulants to mimic the coverage of long-acting versions.
- Dosage Calibration: Transitioning is not a 1:1 ratio; physicians must carefully calculate split doses to avoid “rebound” effects—the sudden return of symptoms as the medication wears off.
- Medical Supervision Required: Self-adjusting medication timing is dangerous. Any switch between stimulant formulations requires a formal titration plan managed by a prescribing clinician.
Pharmacological Mechanisms of Dextroamphetamine
Dextroamphetamine functions by increasing the synaptic concentration of dopamine and norepinephrine, primarily by inhibiting the dopamine transporter (DAT) and norepinephrine transporter (NET). According to the National Institutes of Health (NIH), these neurotransmitters are critical for executive function, focus, and impulse control in individuals with Attention-Deficit/Hyperactivity Disorder (ADHD).

Extended-release (ER) formulations typically utilize a bead-based or osmotic delivery system to provide a steady-state concentration of the drug over 8 to 12 hours. Immediate-release (IR) dextroamphetamine, conversely, enters the bloodstream rapidly, peaking within 1 to 3 hours. The Cureus report highlights that by spacing IR doses throughout the day, clinicians can approximate the steady-state pharmacokinetics of ER drugs, thereby preventing the symptom fluctuation that often triggers patient anxiety during shortages.
Addressing the Supply Chain Crisis in Psychiatry
The U.S. Food and Drug Administration (FDA) has maintained a drug shortage database that has included various ADHD stimulants since late 2022. This ongoing scarcity has forced a shift in clinical practice, moving from ideal, patient-preferred formulations to whatever is currently available in regional pharmacies.

“The challenge with switching to immediate-release stimulants is not just efficacy, but the burden of adherence. Patients must transition from a once-daily regimen to a multi-dose schedule, which significantly increases the risk of missed doses and subsequent symptom breakthrough,” notes Dr. Sarah Jenkins, an independent psychiatric pharmacologist not involved in the study.
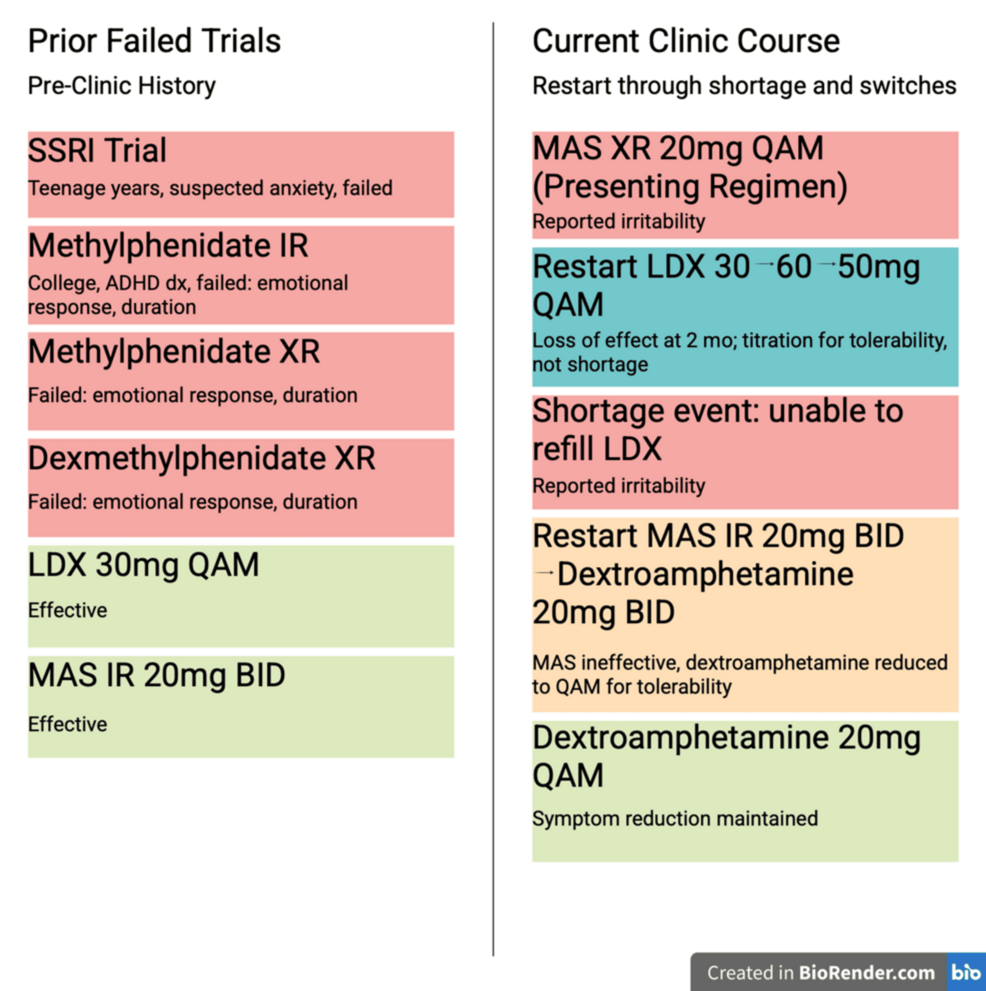
The Cureus case report is notable because it provides a clinical template for physicians navigating these supply chain gaps. By documenting the successful transition of a patient who was experiencing severe ADHD symptoms due to the inability to secure their usual methylphenidate-based ER medication, the authors provide evidence that, with close monitoring, clinical outcomes can be preserved.
| Formulation Type | Mechanism of Delivery | Typical Duration | Primary Clinical Risk |
|---|---|---|---|
| Extended-Release (ER) | Timed-release beads/osmotic | 8–12 Hours | Supply chain instability |
| Immediate-Release (IR) | Rapid absorption | 3–5 Hours | Dose-timing adherence |
Clinical Efficacy and Patient Safety
The study, which was conducted independently and received no external funding from pharmaceutical manufacturers, emphasizes the importance of “metabolic matching.” Because the half-life of IR dextroamphetamine is relatively short, clinicians must account for the “trough” periods—the time between doses where the drug level in the blood drops—to prevent the re-emergence of hyperactivity or inattention.
Research published in The Lancet Psychiatry indicates that while stimulants are highly effective, the risk of cardiovascular side effects, such as increased heart rate or blood pressure, must be monitored regardless of the formulation. Switching to an IR version does not inherently increase these risks, but the frequent dosing schedule requires a high degree of patient compliance.
Contraindications & When to Consult a Doctor
Stimulant medications are contraindicated for patients with symptomatic cardiovascular disease, moderate to severe hypertension, hyperthyroidism, or known hypersensitivity to sympathomimetic amines. Furthermore, patients with a history of substance use disorder or psychosis require strict evaluation before any change in stimulant therapy.
Consult a healthcare provider immediately if you experience:
- Palpitations or chest pain following a dose adjustment.
- Uncontrolled mood swings or severe “crash” symptoms between IR doses.
- New-onset anxiety or sleep disturbances that persist beyond the first week of a new regimen.
Moving Forward: The Future of ADHD Management
As the pharmaceutical industry struggles with production quotas set by the Drug Enforcement Administration (DEA), the Cureus findings provide a pragmatic, albeit temporary, solution. The clinical takeaway remains that while medication flexibility is necessary, the safety profile of stimulants remains unchanged by the formulation switch. Patients should work closely with their providers to map out a dosing schedule that minimizes peak-to-trough fluctuations, ensuring that the necessary treatment for ADHD remains both effective and safe during periods of market instability.

References
- U.S. Food and Drug Administration. (2026). Drug Shortages Database. Retrieved from FDA.gov.
- National Institute of Mental Health. (2023). Attention-Deficit/Hyperactivity Disorder in Adults. NIH Publication.
- Cureus Journal of Medical Science. (2026). Maintained Symptom Control Following a Shortage-Driven Switch to Immediate-Release Dextroamphetamine.
- The Lancet Psychiatry. (2019). Comparative efficacy and tolerability of medications for ADHD.