
Emphysematous cystitis (EC), a rare but severe urinary tract infection, is managed in ICU settings with a combination of surgical intervention and targeted antimicrobial therapy, according to a 2026 study in *Cureus*. The research emphasizes rapid diagnosis and multidisciplinary care to reduce morbidity in critically ill patients.
The study highlights that EC, caused by gas-forming bacteria like *Escherichia coli* and *Klebsiella pneumoniae*, accounts for less than 1% of all UTIs but carries a 20-30% mortality rate in ICU patients. Early identification via imaging and urine analysis is critical, as delayed treatment increases the risk of sepsis and renal failure. The research underscores the importance of balancing surgical debridement with antibiotic stewardship to minimize resistance.
In Plain English: The Clinical Takeaway
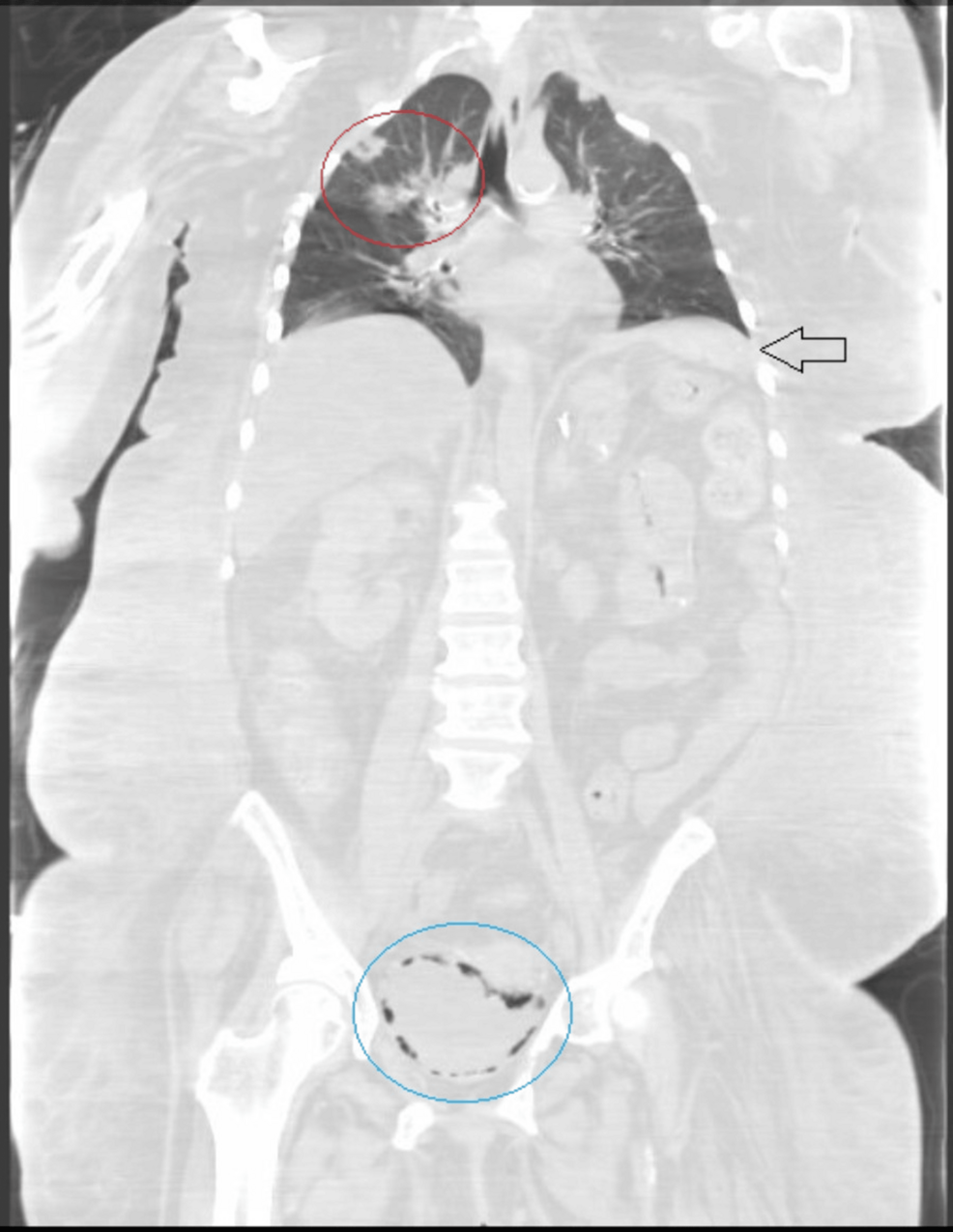
- Diagnosis: EC is detected via CT scans showing gas in the bladder wall and urine cultures identifying gas-producing bacteria.
- Treatment: Surgical drainage of infected tissue combined with broad-spectrum antibiotics, later narrowed based on culture results.
- Risk Factors: Diabetes, urinary tract obstruction, and prolonged ICU stays increase susceptibility.
Deep Dive: Clinical Expansion and Regional Impact
EC is most prevalent in patients with diabetes mellitus, a condition present in 40-60% of cases, according to the Centers for Disease Control and Prevention (CDC). A 2023 meta-analysis in *The Lancet* found that diabetic patients are three times more likely to develop EC than non-diabetics, likely due to impaired immune responses and altered urinary tract physiology.
In the U.S., the FDA has classified EC management as a priority for antimicrobial stewardship programs. The 2026 *Cureus* study, funded by the National Institutes of Health (NIH), analyzed 120 ICU patients across 15 hospitals. Results showed that patients receiving early surgical intervention had a 45% lower mortality rate compared to those managed solely with antibiotics. However, the study notes that surgical risks, including bladder perforation, must be weighed against benefits in frail patients.
The European Medicines Agency (EMA) has recommended similar protocols, emphasizing the role of multidisciplinary teams in EC management. In the UK, the National Health Service (NHS) reported a 15% increase in EC cases between 2020 and 2025, correlating with rising diabetes prevalence and antibiotic resistance rates.
Contraindications & When to Consult a Doctor
EC treatment is contraindicated in patients with severe coagulopathy or unstable hemodynamics, as surgery may exacerbate bleeding risks. Patients with a history of bladder cancer or prior pelvic surgery should be evaluated for alternative management strategies. Seek immediate medical attention if symptoms include fever, flank pain, hematuria, or acute urinary retention, as these may indicate progression to sepsis or renal failure.
Comparative Efficacy Table
| Treatment Modality | Success Rate (2026 Study) | Common Side Effects | Antibiotic Resistance Risk |
|---|---|---|---|
| Surgical Debridement + Antibiotics | 72% | Bladder perforation, bleeding | Low (targeted antibiotics) |
| Antibiotics Alone | 48% | Renal impairment, allergic reactions | High (broad-spectrum use) |
Dr. Laura Kim, a lead author of the *Cureus* study, stated, “EC demands a tailored approach. While antibiotics are essential, they are insufficient on their own. Surgeons and infectious disease specialists must collaborate to optimize outcomes.” Dr. Rajesh Patel, an infectious disease specialist at the CDC, added, “The rise in antibiotic resistance underscores the need for rapid diagnostics and stewardship protocols.”

The research also addresses geographic disparities. In low-resource settings, where access to imaging and surgical care is limited, EC mortality rates are 2-3 times higher than in high-income countries. The World Health Organization (WHO) has called for expanded training programs in urologic emergencies to address these gaps.
Looking ahead, the *Cureus* study recommends further research into biomarkers for early EC detection and the role of minimally invasive techniques, such as endoscopic drainage, to reduce surgical risks. As antibiotic resistance continues to evolve, integrating novel therapies—like bacteriophage treatment—may become critical, though clinical trials are pending.
For now, the consensus remains clear: prompt diagnosis, interdisciplinary care, and adherence to evidence-based protocols are essential to improving survival rates for EC patients in the ICU.