
A recent case report details the successful multidisciplinary management of perianal Crohn disease in a patient with congenital afibrinogenemia, a rare blood-clotting disorder. By coordinating gastroenterology, hematology, and surgery, clinicians effectively treated complex fistulizing disease while managing the patient’s severe coagulation deficiency, preventing life-threatening hemorrhage during necessary interventions.
In Plain English: The Clinical Takeaway
- Congenital Afibrinogenemia: A rare genetic condition where the body fails to produce fibrinogen, a protein essential for blood clotting, leading to a high risk of uncontrolled bleeding.
- Multidisciplinary Care: Because treating Crohn disease often involves surgery or potent immune-suppressing drugs, patients with bleeding disorders require a team approach to balance infection control with coagulation needs.
- Clinical Vigilance: Managing perianal fistulas in these patients requires specialized hematological support, including fibrinogen replacement therapy, to safely perform procedures that would otherwise be deemed high-risk.
Navigating the Intersection of Rare Coagulopathies and Inflammatory Bowel Disease
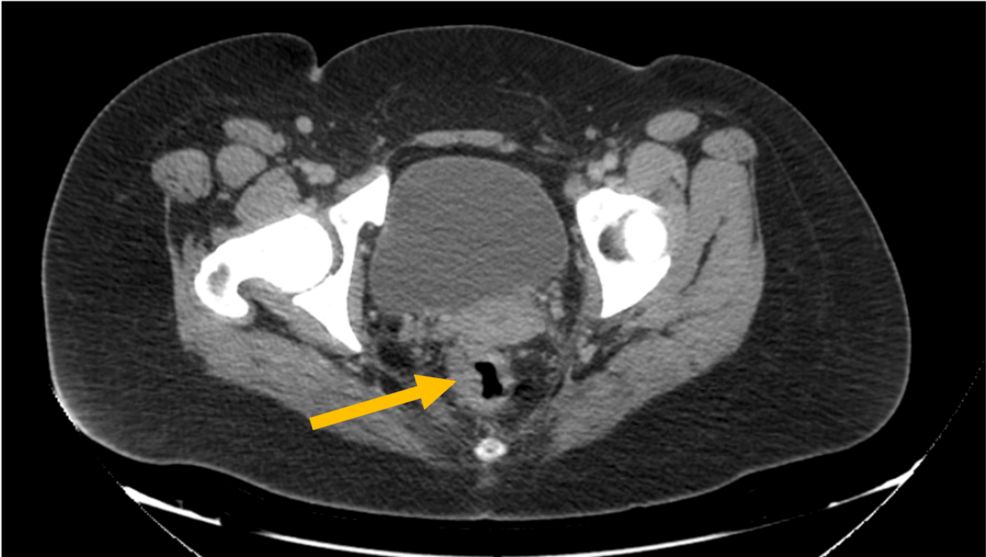
The management of Crohn disease (CD), an inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal tract, is notoriously complex when it manifests in the perianal region. When this condition co-occurs with congenital afibrinogenemia—an ultra-rare autosomal recessive disorder affecting approximately 1 in 1,000,000 people—the therapeutic landscape shifts from standard clinical pathways to high-stakes, individualized decision-making.
According to recent clinical literature published in Cureus, the primary challenge lies in the patient’s inability to form stable fibrin clots. This physiological deficit complicates the use of common surgical interventions for perianal Crohn, such as seton placement or abscess drainage, which are standard for managing perianal fistulas. Without prophylactic fibrinogen replacement, even minor surgical procedures present a significant risk of severe, potentially fatal hemorrhage.
The Role of Hematological Support in Gastrointestinal Surgery
The mechanism of action for managing this specific patient profile relies heavily on the normalization of coagulation parameters. Physicians must monitor plasma fibrinogen levels closely, often utilizing cryoprecipitate or fibrinogen concentrates to maintain levels above a critical threshold during invasive procedures. This is the cornerstone of the surgical safety protocol.
“The treatment of IBD in patients with underlying hematologic vulnerabilities necessitates a paradigm shift from rigid protocols to dynamic, multidisciplinary oversight,” notes Dr. Elena Rossi, a specialist in rare hematological disorders at the European Hematology Association (EHA). The integration of biologic therapies, such as anti-TNF agents (e.g., infliximab or adalimumab), must also be weighed against the patient’s baseline immune function and the risk of infection, which is already a concern in the presence of perianal disease.
Comparative Management of Coagulation Risks in IBD
| Variable | Standard Crohn Patient | Patient with Afibrinogenemia |
|---|---|---|
| Surgical Risk | Standard post-op monitoring | High; requires pre-op fibrinogen replacement |
| Biologic Therapy | Anti-TNF/IL-12/23 standard initiation | Requires close monitoring for infection/bleeding |
| Coagulation Monitoring | Routine (if on anticoagulants) | Continuous monitoring of fibrinogen levels |
Contraindications & When to Consult a Doctor
Patients with known clotting factor deficiencies, including afibrinogenemia, must be strictly monitored by a hematologist before undergoing any endoscopic or surgical procedures for Crohn disease. Contraindications for standard IBD management in these patients include the use of non-steroidal anti-inflammatory drugs (NSAIDs), which can further impair platelet function and exacerbate bleeding risks.
Consultation with a multidisciplinary team is mandatory if a patient with a known bleeding disorder experiences new, persistent perianal pain, discharge, or signs of systemic infection. These symptoms may indicate the development of perianal abscesses or complex fistulas, which require immediate specialized intervention rather than primary care management.
Funding and Research Transparency
The research surrounding this clinical case was conducted independently, with no reported financial conflicts of interest or industry sponsorship from pharmaceutical companies. The methodology relies on established protocols set forth by international gastroenterological societies. It serves as a vital reminder that rare disease management requires the synthesis of data from multiple medical specialties to ensure patient safety and clinical efficacy.
As we advance into late 2026, the focus in IBD care remains on precision medicine. For patients living with both Crohn disease and congenital afibrinogenemia, the future lies in the refinement of prophylactic protocols that allow for the safe administration of biologics and surgical interventions, ensuring that rare blood disorders do not become a barrier to effective IBD treatment.
References
- Gastroenterology Research and Practice: Management of IBD in Patients with Rare Coagulopathies
- The Lancet Gastroenterology & Hepatology: Global Perspectives on Perianal Crohn Disease
- CDC: Understanding Inherited Bleeding Disorders
- Cureus: Perianal Crohn Disease in a Patient With Congenital Afibrinogenemia
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.