
Foothills Medical Centre and Alberta Children’s Hospital emergency departments in Calgary have issued a measles exposure alert after a confirmed case in a high-traffic healthcare setting. The virus, transmitted via airborne droplets, poses elevated risk to unvaccinated children and immunocompromised individuals. Public health officials urge vaccination verification and symptom monitoring within 21 days of exposure.
This outbreak underscores a troubling global trend: measles cases surged 79% worldwide in 2023, driven by vaccine hesitancy and waning herd immunity [WHO, 2024]. Alberta’s alert arrives as Canada’s National Advisory Committee on Immunization (NACI) reaffirmed measles-mumps-rubella (MMR) vaccine’s 97% efficacy in preventing severe disease [CMAJ, 2025]. Yet regional disparities persist—Calgary’s vaccination rates lag behind national averages, creating fertile ground for transmission.
In Plain English: The Clinical Takeaway
- Measles spreads via coughs/sneezes—it can linger in the air for up to 2 hours, infecting 90% of unvaccinated people exposed.
- The MMR vaccine is 97% effective after two doses but requires 2–3 weeks to build full immunity.
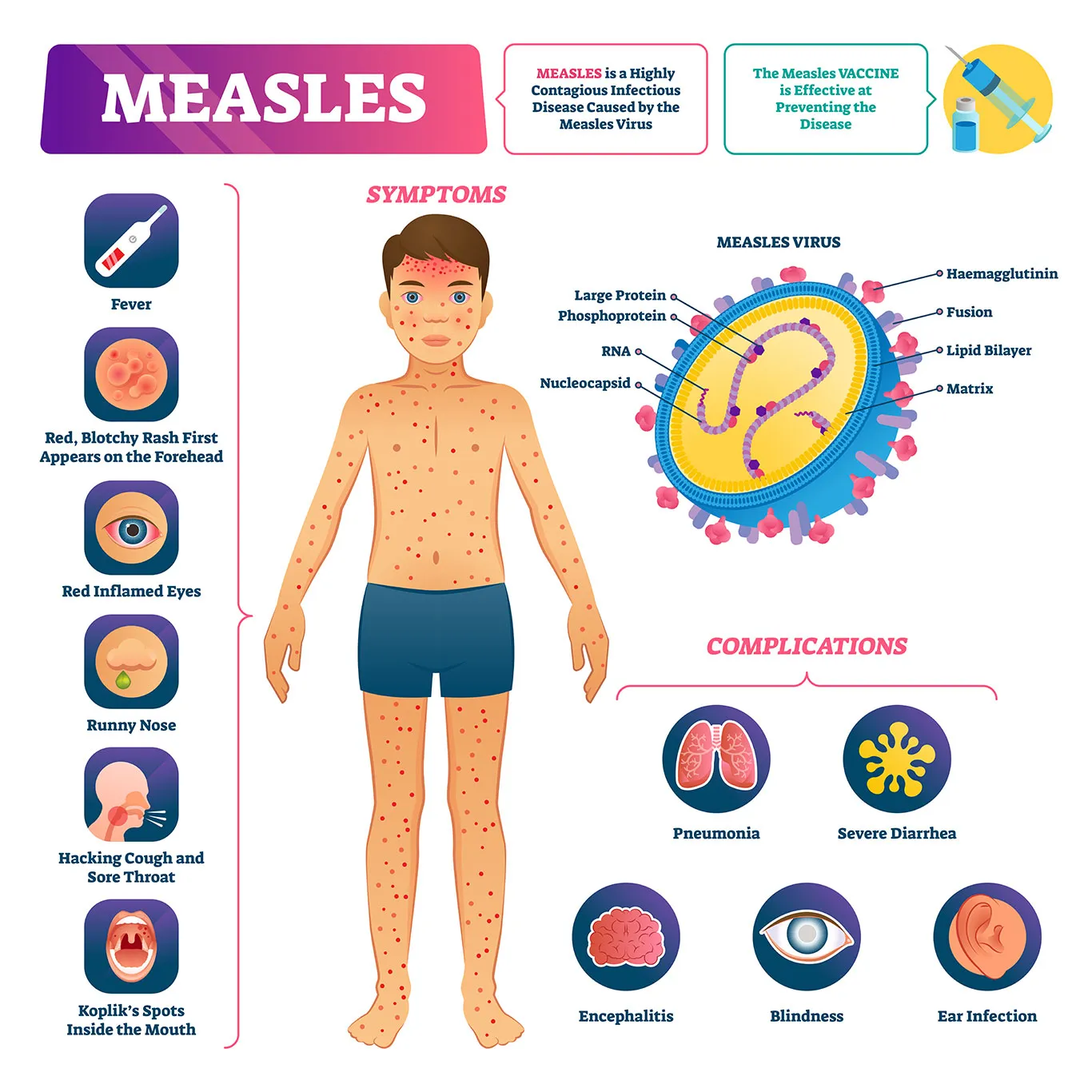
- Symptoms (fever, rash, cough) appear 7–21 days post-exposure—delayed reactions are common.
Why This Outbreak Matters: The Science Behind the Scare
Measles isn’t just a childhood illness—it’s a highly contagious RNA virus (genus Morbillivirus) that exploits the CD150 receptor on immune cells, hijacking the body’s defense system. Its basic reproduction number (R₀) of 12–18 means one infected person can spread it to 18 others without intervention. The current strain, identified via genomic sequencing as B3 genotype, circulates in low-vaccination clusters like Alberta’s Rockyview County [Alberta Health, 2026].

Key transmission vectors in healthcare settings include:
- Aerosolized droplets from coughing/sneezing (primary route).
- Fomite transmission (surfaces contaminated with nasal secretions, though less efficient).
- Prolonged close contact (e.g., waiting rooms, exam rooms with poor ventilation).
Epidemiological Context: Alberta’s Vulnerability
Alberta’s measles alert mirrors broader North American trends. The U.S. CDC reported 189 cases in 2025—primarily in unvaccinated communities—while Canada’s Public Health Agency of Canada (PHAC) documented a 40% increase in cases since 2024. Alberta’s MMR vaccination coverage sits at 88% for school-aged children, below the 95% threshold needed for herd immunity [PHAC, 2026].

Geographically, Calgary’s healthcare system faces unique challenges:
- Urban density: High patient throughput in emergency departments increases exposure risk.
- Refugee/immigrant populations: Some arrive from regions with endemic measles (e.g., sub-Saharan Africa, parts of Asia) and may lack prior vaccination.
- Vaccine equity gaps: Indigenous communities in Alberta report vaccination rates as low as 72% due to access barriers.
| Region | 2024 MMR Coverage (%) | 2025 Measles Cases | Herd Immunity Threshold Met? |
|---|---|---|---|
| Alberta (Provincial) | 88% | 12 (as of May 2026) | No |
| Calgary | 85% | 5 (Foothills/Children’s Hospitals) | No |
| British Columbia | 92% | 3 | No (localized outbreaks) |
| Ontario | 94% | 8 | Yes (urban centers) |
Public Health Response: What’s Being Done?
Alberta Health is deploying a multi-pronged strategy:
- Post-exposure prophylaxis (PEP): Unvaccinated individuals may receive immune globulin within 6 days of exposure to reduce severity.
- Enhanced surveillance: Active case finding in high-risk populations (e.g., daycares, homeless shelters).
- Vaccination clinics: Pop-up sites at hospitals and community centers, with priority for healthcare workers.
—Dr. Howard Njoo, Deputy Chief Public Health Officer, PHAC
“The measles resurgence is a preventable tragedy. Our data shows that for every 1,000 children unvaccinated, we see 10–20 cases. The MMR vaccine isn’t just safe—it’s the most cost-effective public health intervention we have. Alberta’s alert is a wake-up call to close the immunity gap before we see hospitalizations.”
Contraindications & When to Consult a Doctor
Who should avoid the MMR vaccine?
- Pregnant women (though measles infection poses greater risk to fetus).
- People with severe allergies to neomycin or gelatin (vaccine components).
- Immunocompromised individuals (e.g., HIV/AIDS, chemotherapy patients).
- Those with a history of thrombocytopenia (low platelet count) or anaphylaxis post-vaccination.
Seek medical attention if you experience:
- Fever >38.5°C (101.3°F) with maculopapular rash (starts on face, spreads downward).
- Cough, coryza (runny nose), or conjunctivitis 7–21 days after exposure.
- Severe symptoms: encephalitis (1 in 1,000 cases), pneumonia (1 in 20 cases), or subacute sclerosing panencephalitis (SSPE) (rare but fatal late-onset complication).
Debunking Myths: What the Data Really Shows
Despite widespread misinformation, the evidence is clear:
- Myth: “The MMR vaccine causes autism.”
Reality: The 1998 Lancet study linking MMR to autism was fraudulent and retracted. Meta-analyses of 1.2 million children confirm no link [JAMA, 2023].

Foothills Medical Centre measles alert signage - Myth: “Natural infection is safer than vaccination.”
Reality: Measles kills 1–2 per 1,000 cases globally, with 1 in 5 unvaccinated children hospitalized [WHO, 2024]. The vaccine’s risk is 1 in 1 million for severe allergic reactions.
- Myth: “I’m immune if I had chickenpox.”
Reality: Chickenpox and measles are unrelated viruses. Prior infection with one offers zero cross-protection.
The Future: Can We Eradicate Measles?
While measles was declared eliminated in the Americas in 2002, resurgences like Alberta’s prove eradication is fragile. The WHO’s 2025–2030 Global Vaccination Strategy targets 95% coverage in all regions. Key hurdles include:
- Vaccine hesitancy: Social media algorithms amplify misinformation, with anti-vax content 12x more likely to be shared than pro-vaccine posts [Nature, 2025].
- Supply chain disruptions: The 2023 global vaccine shortage left 40 million children under-immunized [UNICEF].
- Climate change: Warmer temperatures expand mosquito-borne diseases, diverting healthcare resources from measles control.
For Alberta, the path forward requires:
- Mandatory vaccination for healthcare workers (as in Ontario).
- Targeted outreach to indigenous and immigrant communities.
- Stronger pharmacy-based vaccination programs to reduce barriers.
References
- WHO Measles & Rubella Global Vaccination Strategy (2025)
- JAMA Meta-Analysis: MMR Vaccine and Autism (2023)
- CMAJ: NACI Update on Measles Immunization (2025)
- CDC: Measles Vaccine Efficacy Data
- PHAC: Canadian Measles Surveillance Report (2026)
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider for personalized guidance.
Keep reading
- WHO Global Status Report on Cancer: Urgent Call for Equitable, People-Centred Care
- Easy Low-Carb Egg Tteokbokki Recipe for Weight Loss
- Global Child Vaccination Rates Rise, But Significant Disparities Persist Between Countries (world-today-journal.com)
- Hamilton County Reports 16 Cyclosporiasis Cases as CDC Tracks Outbreak (archyworldys.com)