
{kind=link}
Medicaid at a Crossroads: Spending Cuts and the Future of Access to Care
A staggering $911 billion. That’s the projected cut to federal Medicaid spending over the next decade, a consequence of recently enacted legislation. This isn’t just a budgetary shift; it’s a potential earthquake for the nearly one in five low-income Americans who rely on Medicaid for healthcare, and a looming challenge for states already grappling with complex healthcare landscapes. The coming years will see significant changes to enrollment, spending per enrollee, and ultimately, access to care – and understanding these shifts is crucial for policymakers, healthcare providers, and individuals alike.
The Looming Impact of Federal Cuts
The new law, signed into law in July, is poised to reshape the Medicaid landscape. While the full impact will unfold over the next ten years, the Congressional Budget Office (CBO) estimates a 14% reduction in federal Medicaid spending and a projected increase of 10 million uninsured Americans, many of whom will lose Medicaid coverage. Crucially, over half of these cuts will disproportionately affect states that expanded Medicaid under the Affordable Care Act (ACA). This creates a two-tiered impact, with expansion states facing steeper reductions and potentially more significant enrollment declines.
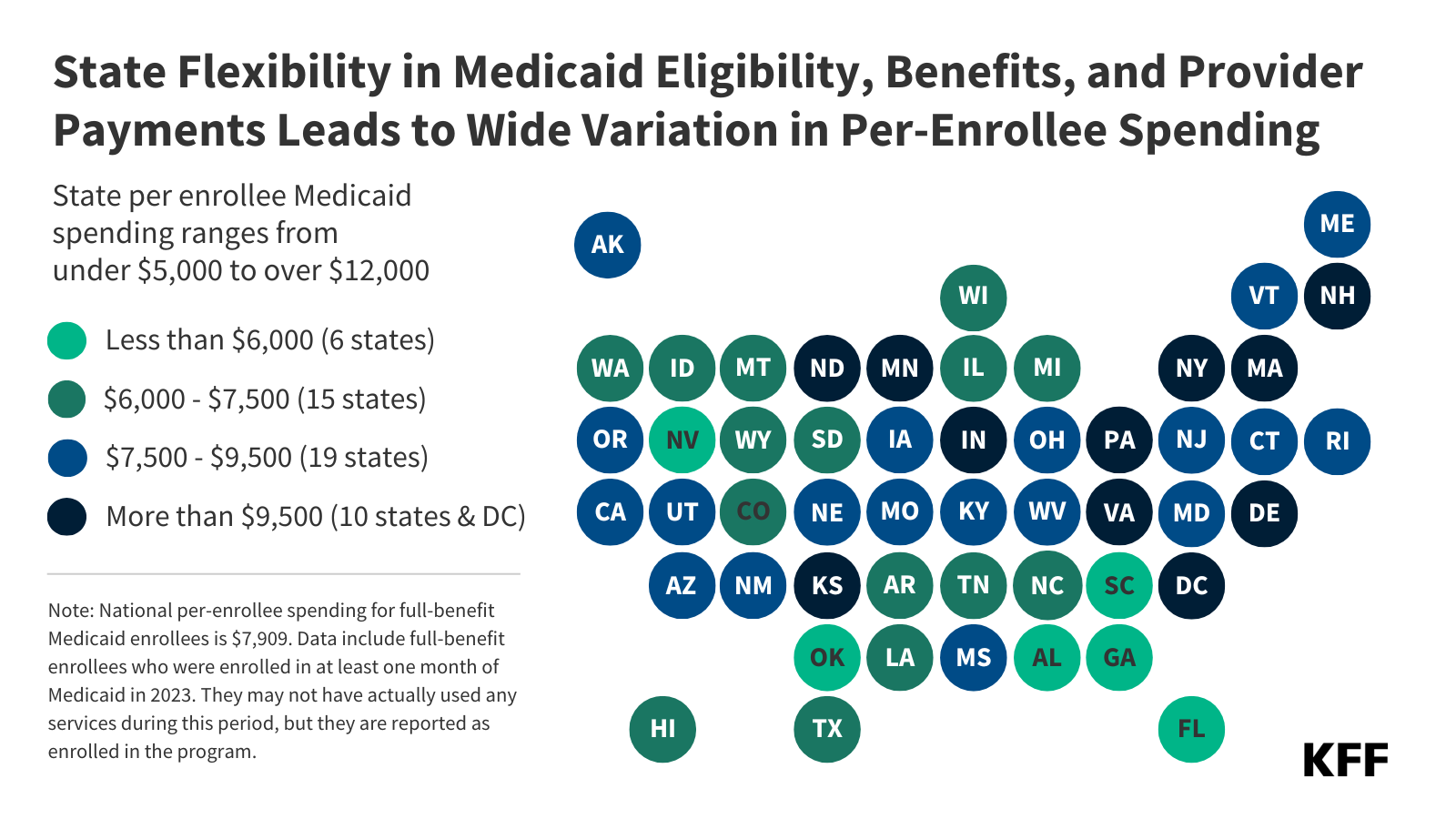
How states respond to these funding reductions will be critical. Will they cut benefits, restrict eligibility, or seek alternative funding sources? The answers will vary widely, leading to a patchwork of changes across the country. This variability is inherent in the Medicaid system, as states retain considerable flexibility in program design within federal guidelines, resulting in significant differences in spending and enrollment.
Uneven Spending: A State-by-State Breakdown
Currently, national Medicaid spending per enrollee stands at $7,909, but this figure masks substantial disparities. States like Alabama, Florida, Georgia, and Nevada consistently report some of the lowest per-enrollee spending, while Washington, D.C., Minnesota, Pennsylvania, and North Dakota are at the higher end, exceeding $10,000 per enrollee in some cases. These differences aren’t arbitrary. They reflect variations in state demographics, revenue-raising capacity, healthcare costs, and policy choices.
These state-level variations extend to specific eligibility groups. Individuals with disabilities and older adults consistently represent the highest per-enrollee spending – $20,950 and $20,194 respectively – due to their more complex healthcare needs and higher rates of chronic conditions. Children, on the other hand, have the lowest per-enrollee spending at $3,321. This disparity highlights the need for targeted approaches to Medicaid funding and resource allocation.
The Dual-Eligible Challenge and Long-Term Care Costs
A significant factor driving up per-enrollee spending is the prevalence of dual eligibility – individuals who qualify for both Medicaid and Medicare. For these individuals, Medicaid often covers services that Medicare doesn’t, such as vision, dental, and crucially, long-term care (LTC). States have significant discretion over LTC coverage, leading to wide variations in spending. Minnesota, for example, spends $57,900 per enrollee with disabilities, while Florida spends just $5,040 – a difference largely attributable to differing LTC policies.
As the population ages, the demand for LTC will only increase, placing further strain on Medicaid budgets. States will need to proactively address LTC financing and delivery models to ensure sustainable access to care for vulnerable populations. This could involve exploring innovative approaches like home and community-based services, which can often be more cost-effective than institutional care.
Medicaid Expansion and Spending Patterns
Interestingly, states that expanded Medicaid under the ACA actually spend more per enrollee than non-expansion states – $8,444 versus $7,591. This challenges the notion that expansion simply shifts costs without improving care. In fact, expansion states spend more per enrollee across all eligibility groups, including those not directly related to the expansion population. This suggests that expansion may be associated with broader investments in healthcare infrastructure and improved access to care.
However, the looming federal cuts threaten to undermine these gains. The 90% federal match rate for expansion adults, while initially beneficial, may have incentivized states to prioritize services for this group. As federal funding decreases, states may be forced to make difficult choices about which services to maintain and which to cut.
What’s Next for Medicaid?
The future of Medicaid is uncertain. The combination of federal spending cuts, increasing healthcare costs, and an aging population presents a formidable challenge. States will need to become more efficient in their Medicaid administration, explore innovative care delivery models, and potentially seek alternative funding sources. The wide variation in spending across states also presents an opportunity for learning and collaboration – states with successful cost-containment strategies can serve as models for others.
Ultimately, the fate of Medicaid will have profound implications for millions of Americans. Protecting access to affordable healthcare for low-income individuals is not only a moral imperative but also a critical investment in the nation’s health and economic well-being. KFF (Kaiser Family Foundation) provides comprehensive data and analysis on Medicaid and healthcare policy. What strategies will states employ to navigate these turbulent waters? Share your thoughts in the comments below!