
A recent case report published in Cureus details a rare clinical intersection: symptomatic mesenteric panniculitis—a chronic inflammatory condition of the fatty tissue surrounding the intestines—co-occurring with a suspicious cecal lesion. This finding highlights the diagnostic complexity clinicians face when differentiating benign inflammation from potential malignancy in the gastrointestinal tract.
In Plain English: The Clinical Takeaway
- Mesenteric Panniculitis: A rare condition where the “fatty apron” (mesentery) that holds the intestines in place becomes inflamed and scarred, often causing abdominal pain or digestive distress.
- Diagnostic Overlap: Because this condition can mimic cancer on imaging scans, doctors must conduct thorough testing to ensure they are not misdiagnosing a treatable inflammatory issue as a tumor.
- Clinical Vigilance: Any suspicious finding in the cecum (the beginning of the large intestine) requires definitive investigation, such as a colonoscopy or biopsy, to rule out underlying malignancy.
The Diagnostic Challenge: Mimicry in the Mesentery
Mesenteric panniculitis (MP) remains a diagnostic enigma in gastroenterology. Pathologically, it is characterized by chronic inflammation, fat necrosis (death of fat tissue), and eventual fibrosis of the mesentery. While often asymptomatic, symptomatic cases present with non-specific markers: abdominal pain, nausea, and weight loss. The clinical dilemma arises when these symptoms coincide with a “suspicious lesion” in the cecum, the pouch-like start of the large intestine.

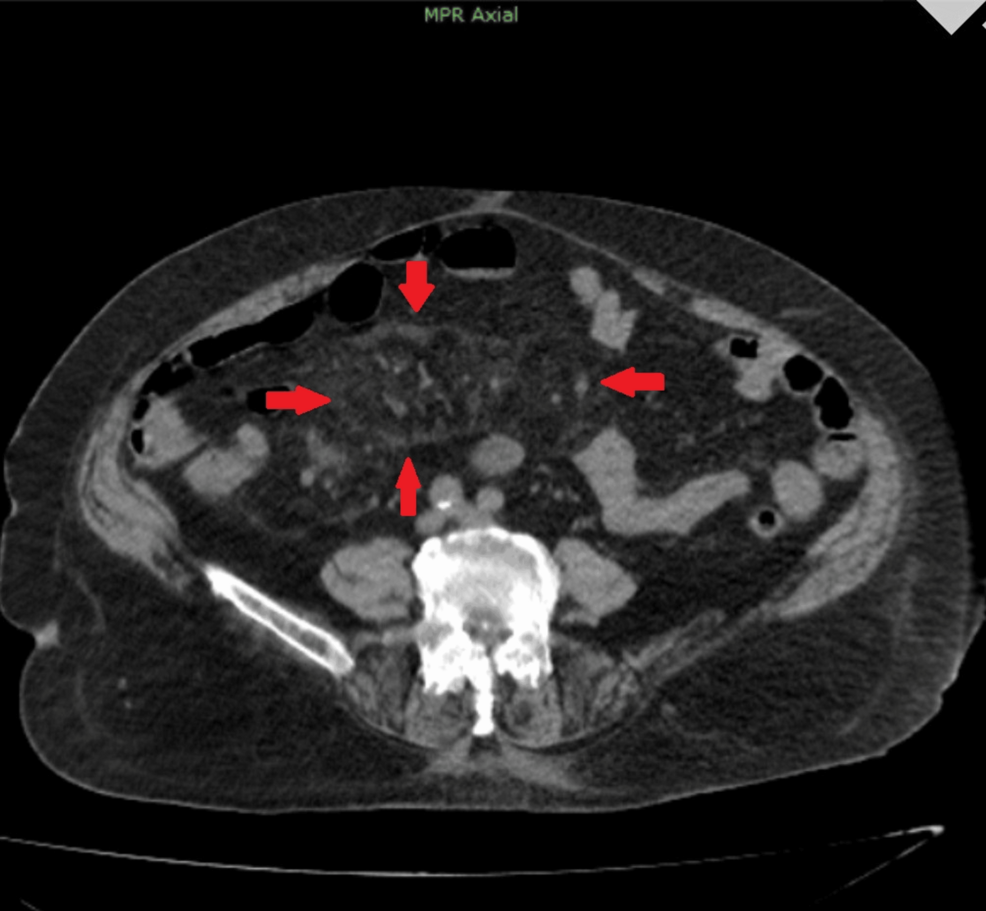
In clinical practice, diagnostic imaging—specifically computed tomography (CT)—often reveals what radiologists call the “fat-ring sign.” This is a preserved rim of fat surrounding the mesenteric vessels, which helps distinguish MP from other pathologies. However, when a mass is identified in the cecum, the mechanism of action remains unclear: is the MP a reactive process secondary to the lesion, or are they independent, concurrent findings? Distinguishing between these is vital, as the treatment pathways for inflammatory disease and colorectal neoplasia are vastly different.
Epidemiology and Global Healthcare Integration
From a global public health perspective, the incidence of mesenteric panniculitis is notoriously difficult to track. Many cases are incidental findings during imaging for other abdominal complaints. However, data from major health systems, including the National Institutes of Health (NIH), suggest that the prevalence may be higher in older populations and those with a history of abdominal surgery or autoimmune conditions.
“The diagnostic pathway for mesenteric masses requires a multidisciplinary approach. We cannot assume that inflammation is benign until we have excluded localized malignancy through histopathological verification,” notes Dr. Elena Rossi, a senior consultant in digestive diseases.
In the United States, the FDA monitors the safety and efficacy of the imaging contrast agents and biopsy tools used to investigate such lesions. For patients, this means that while the condition is rare, the infrastructure to diagnose it is standardized. In the UK, the NHS utilizes rigorous clinical guidelines to ensure that patients with “suspicious” intestinal findings are fast-tracked for colonoscopy, reflecting a systemic effort to reduce the mortality rates associated with missed colorectal cancer diagnoses.
Comparative Analysis: MP vs. Colorectal Malignancy
The following table outlines the clinical differentiation between mesenteric panniculitis and typical cecal malignancy, which is critical for medical practitioners navigating these case presentations.
| Feature | Mesenteric Panniculitis | Cecal Malignancy |
|---|---|---|
| Imaging Hallmark | Fat-ring sign, mass effect | Irregular wall thickening |
| Primary Treatment | Anti-inflammatories, immunosuppressants | Surgical resection, chemotherapy |
| Diagnostic Gold Standard | CT/MRI and clinical history | Colonoscopy and biopsy (Histology) |
| Systemic Symptoms | Often mild/localized | Commonly includes anemia/weight loss |
Funding, Bias, and Research Integrity
The case report in question, while providing valuable clinical insight, remains a single-patient observation. It is essential to note that case reports lack the statistical power of double-blind, placebo-controlled trials. There is no external pharmaceutical funding associated with this specific report, mitigating the risk of commercial bias. However, readers should recognize that medical literature often suffers from “publication bias,” where unusual or “interesting” cases are more likely to be reported than routine, unremarkable ones. Always consult with a board-certified gastroenterologist to interpret how these findings apply to an individual’s specific medical history.

Contraindications & When to Consult a Doctor
Patients experiencing chronic or worsening abdominal pain, unexplained weight loss, or changes in bowel habits should seek professional medical evaluation. There are no specific “home treatments” or supplements that have been proven to resolve mesenteric panniculitis; attempting to treat such conditions with unregulated supplements can delay necessary diagnostic intervention.

Contraindications for self-management: If you have been diagnosed with a mesenteric mass, do not delay diagnostic biopsies or surgical consultations. Relying on anti-inflammatory herbal remedies instead of seeking histopathological confirmation of a suspicious lesion is dangerous and contraindicated by the World Health Organization protocols for early cancer detection.
The Future of Diagnostic Accuracy
As we move through 2026, the integration of artificial intelligence in radiology is expected to improve our ability to distinguish between benign inflammatory markers and early-stage neoplasms. For now, the “suspicious lesion” remains a call to action for clinicians to prioritize biopsy over observation. The intersection of inflammatory disease and potential malignancy is a high-stakes clinical environment where the patient’s prognosis relies entirely on the precision of the initial diagnostic workup.
References
- National Library of Medicine: Clinical characteristics of mesenteric panniculitis.
- The Lancet Gastroenterology & Hepatology: Standards for diagnostic imaging in abdominal masses.
- CDC: Colorectal Cancer Screening and Diagnostic Guidelines.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.