
Metabolic dysfunction-associated steatotic liver disease (MASLD) is projected to affect 1.8 billion people globally by 2050. Driven by rising obesity and type 2 diabetes, this silent epidemic increases risks of cirrhosis and liver cancer, necessitating urgent systemic screening and metabolic intervention across global healthcare infrastructures.
The scale of this projection, highlighted in recent clinical discussions and reports from the American Journal of Managed Care, represents a seismic shift in global hepatology. We are moving from a world where liver failure was primarily associated with alcohol misuse or viral hepatitis to one where metabolic health—or the lack thereof—is the primary driver of organ failure. This is not merely a statistical trend; it is a public health crisis that threatens to overwhelm transplant lists and healthcare budgets from the NHS in the UK to the fragmented systems of the United States.
In Plain English: The Clinical Takeaway
- The Silent Rise: Fatty liver disease is no longer just about alcohol; it is now closely linked to metabolic syndrome (obesity, high blood pressure, and high blood sugar).
- The Hidden Danger: Most people have no symptoms until the liver is severely scarred (cirrhosis), meaning early screening is the only way to prevent permanent damage.
- The Good News: In its early stages, this condition is often reversible through targeted weight loss and metabolic management.
The Pathophysiology of Metabolic Dysfunction-Associated Steatotic Liver Disease
To understand the trajectory toward 1.8 billion cases, we must examine the mechanism of action—the biological process by which the disease develops. MASLD begins with the accumulation of triglycerides in the liver cells, a process known as steatosis. While simple fat accumulation is often benign, a subset of patients progresses to Metabolic Dysfunction-Associated Steatohepatitis (MASH).

MASH involves an inflammatory response and cellular injury. This triggers fibrosis, the formation of excess fibrous connective tissue (scarring). When fibrosis becomes extensive, it leads to cirrhosis, where the liver can no longer perform vital functions like detoxifying blood or producing clotting proteins. This progression is fueled by insulin resistance, which disrupts the body’s ability to regulate glucose and lipids, effectively “flooding” the liver with fat.
The transition from MASLD to MASH is the critical clinical tipping point. Current research focuses on the gut-liver axis, exploring how imbalances in gut microbiota can trigger systemic inflammation that accelerates liver scarring. By targeting these pathways, researchers hope to move beyond lifestyle advice toward pharmacological interventions that can actually “reverse” fibrosis.
Global Epidemiological Shifts and Regulatory Hurdles
The geographic distribution of this surge is not uniform. While North America and Europe have seen a steady climb, the most aggressive increases are now occurring in Asia and the Middle East due to rapid “Westernization” of diets and sedentary lifestyles. This creates a massive burden on regional health systems, such as the World Health Organization (WHO) member states in developing economies where liver biopsy tools are scarce.
From a regulatory standpoint, the FDA and EMA are facing pressure to approve the first wave of targeted therapies. For years, the “gold standard” for diagnosis was the liver biopsy—an invasive procedure. However, the shift toward non-invasive biomarkers (like the FIB-4 index or FibroScan) is essential for the mass screening required to manage a population of nearly 2 billion people.
“The global burden of metabolic liver disease is escalating at a rate that exceeds our current diagnostic capacity. We are facing a ‘silent pandemic’ where the lack of early symptoms masks a progressive pathology that will define the next three decades of gastroenterology.”
The funding for these large-scale epidemiological studies often comes from a mix of governmental health agencies and pharmaceutical consortia. While industry funding accelerates drug development for MASH, it can create a bias toward pharmacological solutions over primary prevention and public health policy changes regarding processed sugar and urban planning.
| Disease Stage | Clinical Characteristics | Primary Risk Factor | Reversibility |
|---|---|---|---|
| MASLD (Steatosis) | Fat accumulation in hepatocytes | Insulin Resistance | High (via lifestyle) |
| MASH (Steatohepatitis) | Inflammation + Ballooning | Metabolic Syndrome | Moderate (pharmacological/diet) |
| Advanced Fibrosis | Significant scarring of tissue | Chronic Inflammation | Low (stabilization focus) |
| Cirrhosis | Widespread nodular regeneration | End-stage organ failure | Very Low (Transplant required) |
Closing the Information Gap: The Role of GLP-1 Agonists
While the source materials emphasize the numbers, they often omit the current pharmaceutical frontier: GLP-1 receptor agonists. Originally designed for diabetes and weight loss, these drugs are showing significant promise in reducing liver fat. By improving insulin sensitivity and reducing systemic inflammation, they address the root cause of the metabolic surge.
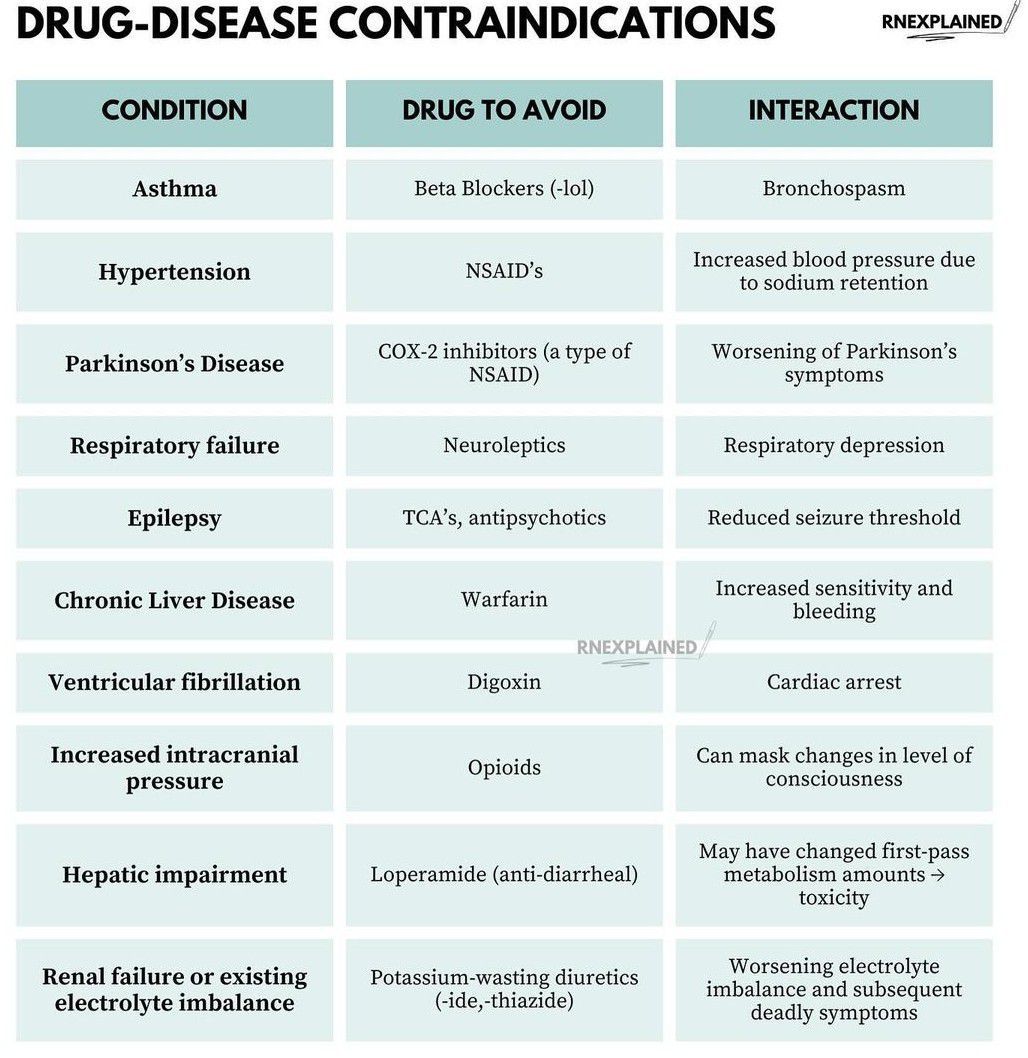
However, the contraindications (reasons a person should not use a drug) are vital. Patients with a history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome should avoid these agents. The high cost of these medications creates a “care gap,” where only affluent populations in the US or EU can access the most effective metabolic interventions, while the 1.8 billion projected cases will largely occur in regions with limited drug access.
Contraindications & When to Consult a Doctor
Lifestyle interventions are the first line of defense, but they are not universal. Individuals with advanced heart failure or severe kidney disease must consult a physician before attempting rapid weight loss or starting high-intensity exercise regimens, as these can place undue stress on the cardiovascular system.
Try to seek immediate medical evaluation if you experience the following “red flag” symptoms of advanced liver dysfunction:
- Jaundice: Yellowing of the skin or the whites of the eyes.
- Ascites: Sudden, unexplained swelling in the abdomen.
- Hepatic Encephalopathy: Confusion, disorientation, or extreme drowsiness.
- Easy Bruising: Unexplained bleeding or bruising due to decreased clotting factor production.
The Path Forward: From Reaction to Prevention
The projection of 1.8 billion people by 2050 is a warning, not a destiny. The trajectory can be altered through a dual-track approach: aggressive primary prevention via public health policy (e.g., sugar taxes and urban walkability) and the implementation of non-invasive screening in primary care settings.
If we continue to rely on “waiting for symptoms” to diagnose liver disease, we are essentially waiting for the disease to become irreversible. The future of hepatology must be translational—moving the science from the peer-reviewed journal into the community clinic, ensuring that metabolic health is treated as a systemic priority rather than an individual failure.
References
- PubMed National Library of Medicine – Research on MASLD/MASH progression and biomarkers.
- The Lancet – Global burden of liver disease and epidemiological trends.
- Centers for Disease Control and Prevention (CDC) – Guidelines on metabolic syndrome and obesity management.
- World Health Organization (WHO) – Global reports on non-communicable diseases (NCDs).