
Mycosis fungoides (MF), the most common form of cutaneous T-cell lymphoma, is a rare malignancy of the immune system where T-cells become cancerous and infiltrate the skin. Recent clinical documentation emphasizes the diagnostic challenges of this condition, which often mimics benign dermatological issues, leading to delayed therapeutic intervention.
In Plain English: The Clinical Takeaway
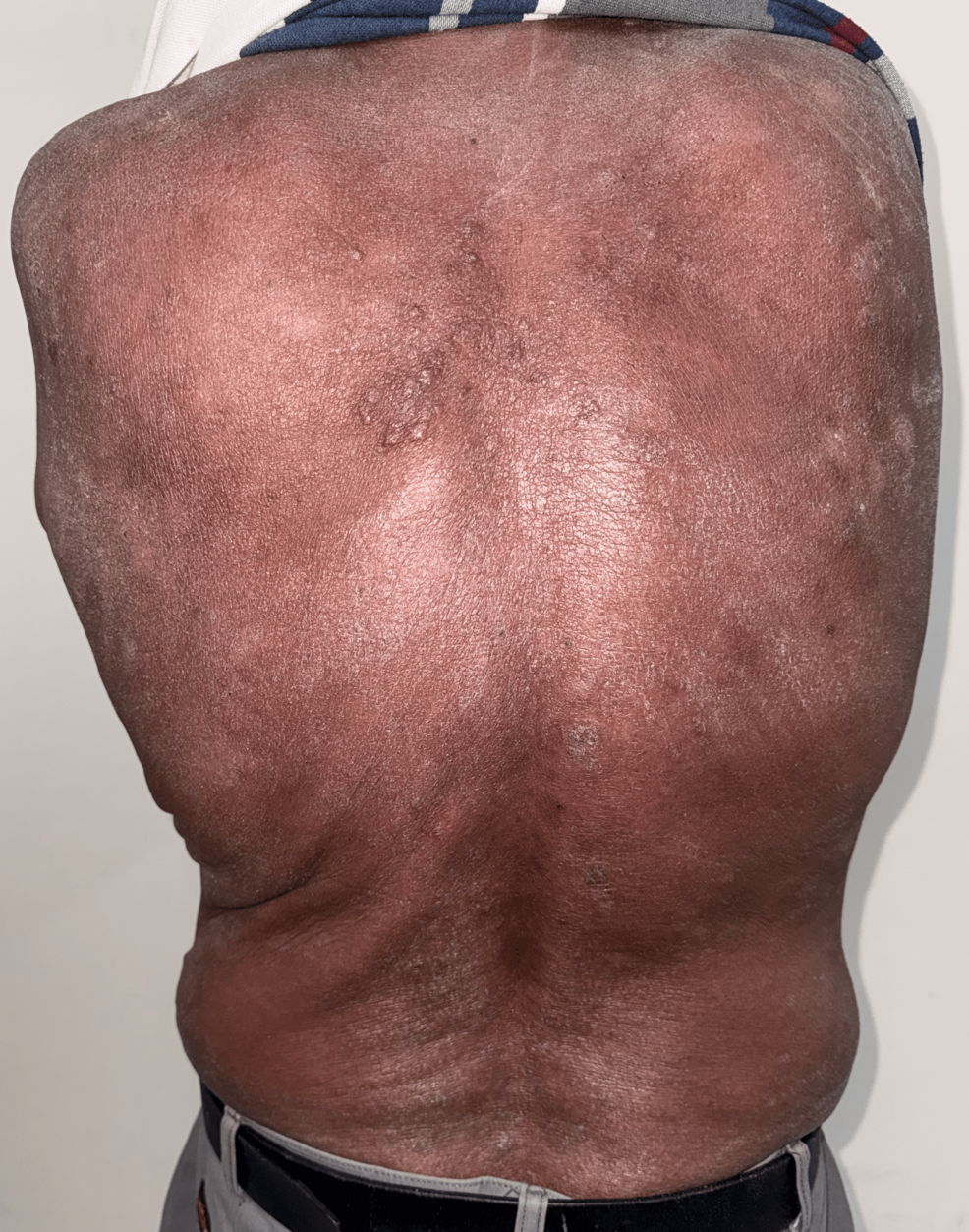
- The Mimicry Problem: MF frequently presents as persistent patches or plaques that look like eczema or psoriasis, often causing significant delays in receiving an accurate diagnosis.
- Staging Matters: Treatment is highly dependent on whether the disease is confined to the skin or has progressed to the lymph nodes or internal organs.
- Multidisciplinary Care: Management requires a team, typically involving dermatologists, oncologists, and radiation specialists, to ensure the right balance of topical and systemic therapies.
The Diagnostic Complexity of Cutaneous T-Cell Lymphoma
Mycosis fungoides represents a specific subtype of non-Hodgkin lymphoma. Unlike typical lymphomas that originate in the lymph nodes, MF begins in the skin. According to the National Cancer Institute, the disease often progresses through distinct stages: the patch stage (thin, red, scaly skin), the plaque stage (thicker, raised lesions), and the tumor stage. The primary clinical challenge is the “diagnostic latency”—the time between initial symptom onset and histopathological confirmation—which can span years.
The recent case report published in Cureus highlights that even with modern diagnostic tools, distinguishing MF from inflammatory dermatoses remains difficult. Histopathology, which involves examining skin tissue under a microscope, is the gold standard. However, early-stage MF often lacks the classic Pautrier’s microabscesses (small pockets of cancerous cells in the skin layers), necessitating repeated biopsies and immunohistochemistry to identify the specific T-cell receptor expression.
Clinical Data and Therapeutic Landscape
Current management strategies for MF are dictated by the TNMB classification system (Tumor, Node, Metastasis, Blood). For early-stage disease, skin-directed therapies such as topical corticosteroids, phototherapy (narrowband UVB), or topical chemotherapy like mechlorethamine are first-line interventions. Systemic therapies, including histone deacetylase (HDAC) inhibitors or extracorporeal photopheresis, are reserved for advanced or refractory cases.
| Treatment Category | Primary Mechanism of Action | Typical Application |
|---|---|---|
| Phototherapy (NBUVB) | Induces apoptosis in malignant T-cells via UV radiation | Early-stage (IA-IIA) |
| Topical Mechlorethamine | Alkylating agent; disrupts DNA synthesis in skin cells | Patch/Plaque stage |
| HDAC Inhibitors | Alters gene expression to halt cancer cell proliferation | Advanced/Refractory cases |
Bridging Research to Global Healthcare Access
The transition from clinical trial data to clinical practice is governed by regional bodies such as the FDA (United States) and the EMA (Europe). While specialized centers have access to targeted therapies, the broader medical community often struggles with identifying MF early. As noted by Dr. Alain Rook, a leading expert in cutaneous lymphoma at the University of Pennsylvania, “The greatest challenge in MF management remains the initial clinical suspicion; physicians must maintain a low threshold for biopsy in patients with chronic, treatment-resistant rashes.”
Funding for research into this rare malignancy often comes from a combination of government grants (such as the NIH) and pharmaceutical industry-sponsored trials. Transparency in these disclosures is vital, as clinical trials for orphan diseases often involve small N-values, making statistical significance harder to achieve compared to common solid tumors.
Contraindications & When to Consult a Doctor
Patients currently managing dermatological symptoms should be aware of specific warning signs that warrant an urgent oncology consultation. If a persistent rash fails to respond to standard topical steroids after 4 to 8 weeks, a biopsy is medically indicated.
Contraindications for certain MF treatments include:
- Phototherapy: Patients with a history of photosensitivity disorders or xeroderma pigmentosum.
- Topical Chemotherapy: Not recommended for patients with extensive ulcerated lesions or those with severe contact dermatitis to the specific agent.
- Systemic Immunotherapy: Patients with active, uncontrolled systemic infections or severe autoimmune comorbidities require careful risk-benefit stratification.
Always seek professional dermatological evaluation if you observe “patchy” lesions that are migrating, thickening, or accompanied by unexplained pruritus (severe itching) or lymphadenopathy (swollen lymph nodes).
The Future Trajectory of MF Research
The integration of molecular profiling into standard diagnostic workups is the next frontier. By identifying specific genetic mutations within the T-cell clones, researchers hope to develop personalized therapeutic regimens that minimize systemic toxicity. While MF remains a chronic, often incurable condition for many, advancements in immunotherapy and targeted biologics are significantly improving the quality of life and progression-free survival rates for patients worldwide.
References
- National Cancer Institute: PDQ Cancer Information Summaries (Mycosis Fungoides)
- The Lancet Oncology: Advances in the Management of Cutaneous T-cell Lymphoma
- Cureus: Journal of Medical Science (Peer-Reviewed Case Reports)
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of a board-certified physician or other qualified health provider with any questions regarding a medical condition.