
Aging populations globally face a critical rise in musculoskeletal degeneration. Optimizing nutrition—specifically protein, calcium, and vitamin D intake—is essential to mitigate osteoporosis and osteoarthritis, reducing fracture risks and preserving mobility in elderly patients through evidence-based dietary interventions and clinical supplementation.
For the aging patient, the intersection of nutrition and bone health is not merely about “eating well”; We see about managing the systemic decline of bone mineral density (BMD) and the degradation of articular cartilage. As we move into mid-April 2026, the clinical focus has shifted from simple supplementation to “precision nutrition,” where dietary intake is calibrated against specific biomarkers of bone resorption. When nutrition fails, the result is a cascade of fragility fractures that drastically increase morbidity and mortality in the elderly.
In Plain English: The Clinical Takeaway
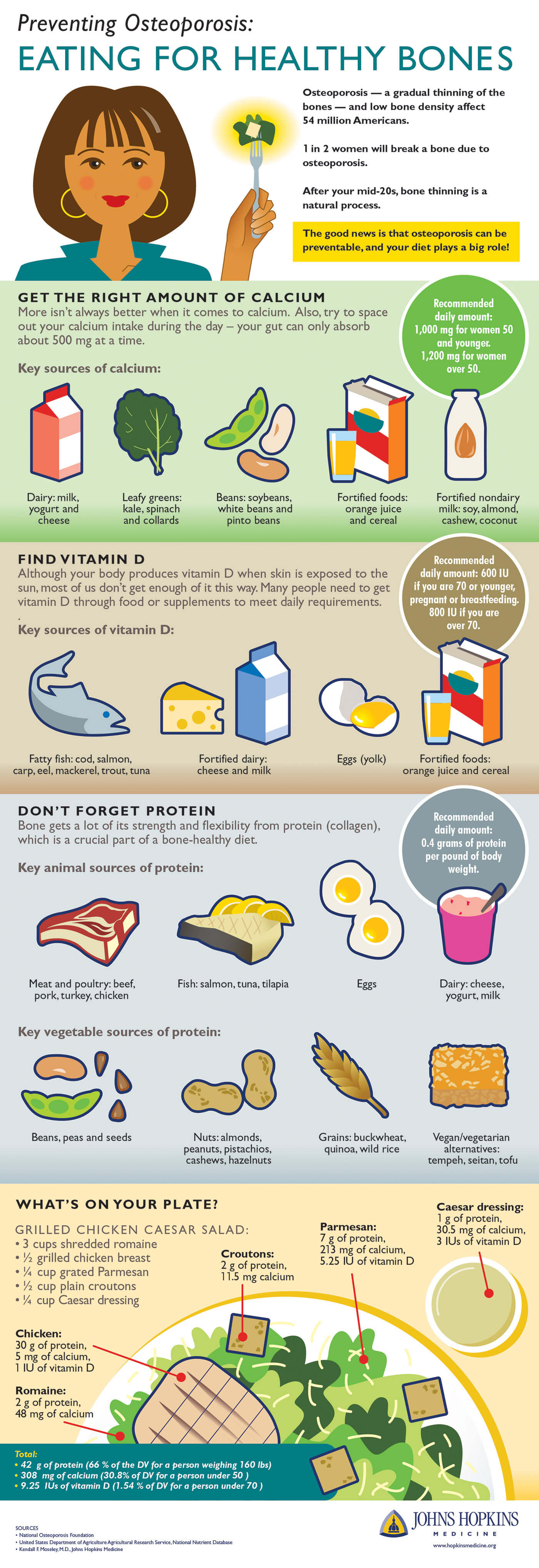
- Protein is a Pillar: It is not just for muscles; protein provides the structural matrix that holds calcium in your bones.
- The Vitamin D-Calcium Axis: Calcium is the “brick,” but Vitamin D is the “mortar” that allows your body to actually absorb that calcium.
- Preventative Movement: Nutrition only works if paired with weight-bearing exercise, which signals the bones to strengthen.
The Molecular Mechanism of Bone Resorption and Nutritional Interference
To understand why nutrition is critical, we must examine the mechanism of action—the specific biological process—of bone remodeling. Bone is a living tissue constantly being broken down by osteoclasts and rebuilt by osteoblasts. In older adults, this balance shifts toward resorption (breakdown), leading to osteoporosis.

Clinical evidence suggests that a deficiency in protein leads to a decrease in Insulin-like Growth Factor 1 (IGF-1), which is vital for osteoblast activity. When protein intake drops, the bone matrix becomes porous. The synergy between Calcium and Vitamin D is non-negotiable. Without sufficient Vitamin D, the intestines cannot efficiently absorb calcium, leading the body to “steal” calcium from the skeleton to maintain blood levels, further weakening the bone structure.
“The challenge in geriatric nutrition is not just the availability of nutrients, but the bioavailability. Age-related declines in gastric acid secretion and intestinal absorption mean that the elderly require higher-quality, more bioavailable forms of nutrients to maintain skeletal integrity.” — Dr. Sarah Jenkins, Lead Epidemiologist in Geriatric Health.
Global Healthcare Integration and Regional Access
The approach to geriatric bone health varies significantly by regulatory region. In the United States, the FDA focuses heavily on the regulation of calcium and vitamin D supplements, often warning against excessive intake that can lead to hypercalcemia (too much calcium in the blood). In contrast, the NHS in the UK emphasizes a “food-first” approach, integrating community-based nutritional support into primary care to prevent falls.
In East Asia, particularly South Korea, there is an increasing clinical emphasis on the “Sarcopenia-Osteoporosis” link—the simultaneous loss of muscle and bone mass. This has led to the development of specialized medical nutrition drinks that combine high-leucine protein with vitamin D, aimed at reducing the high rate of hip fractures seen in urban elderly populations.
Regarding funding and transparency, much of the current longitudinal data on protein supplementation is funded by independent university grants and public health agencies (such as the NIH), though some specific supplement trials are industry-funded. It is imperative that clinicians distinguish between generic nutritional guidelines and product-specific marketing.
Comparative Nutritional Requirements for Bone Maintenance
The following table outlines the evidence-based targets for elderly patients to prevent the progression of bone and joint disease, based on current clinical consensus.
| Nutrient | Clinical Target (Daily) | Primary Function | Risk of Deficiency |
|---|---|---|---|
| Protein | 1.2 – 1.5g / kg body weight | Collagen synthesis & muscle mass | Sarcopenia & fragility fractures |
| Calcium | 1,000 – 1,200 mg | Bone mineral density (BMD) | Osteoporosis |
| Vitamin D | 800 – 2,000 IU | Calcium absorption | Osteomalacia & muscle weakness |
| Omega-3 | 250 – 500 mg | Reduction of joint inflammation | Accelerated osteoarthritis |
The Synergy of Nutrition and Pharmacological Intervention
Nutrition is the foundation, but for patients with established osteoporosis, it must be paired with pharmacotherapy. The use of bisphosphonates—drugs that slow the rate of bone loss—is common. However, these medications can have contraindications (conditions where the drug should not be used), such as severe renal impairment. If a patient is taking bisphosphonates without adequate calcium and vitamin D, the drug’s efficacy is significantly diminished due to the fact that the body lacks the raw materials to rebuild the bone.
Recent double-blind placebo-controlled trials—the gold standard of research where neither the patient nor the doctor knows who receives the treatment—have shown that combining high-protein diets with resistance training reduces the risk of falls by up to 30% compared to nutrition alone. This underscores the necessity of a multidisciplinary approach involving dietitians, physiotherapists, and endocrinologists.
Contraindications & When to Consult a Doctor
While nutritional optimization is generally safe, certain individuals must exercise caution. Patients with chronic kidney disease (CKD) must avoid high-protein diets and excessive calcium supplementation, as their kidneys cannot efficiently clear phosphate and calcium, which can lead to dangerous calcification of the arteries.
You should consult a physician immediately if you experience:
- A sudden loss of height (more than 1.5 inches), which may indicate a vertebral compression fracture.
- Severe joint swelling accompanied by fever, which suggests an inflammatory or infectious process rather than simple osteoarthritis.
- Persistent muscle weakness that prevents standing from a seated position without assistance.
- Hypercalcemia symptoms, such as nausea, constipation, or confusion, which can occur from over-supplementation.
The future of geriatric bone health lies in the transition from general guidelines to personalized nutrition. By monitoring biomarkers and tailoring protein and mineral intake, we can move beyond merely treating fractures to actively preserving the independence and quality of life for the global elderly population.