

The Democratic Republic of Congo’s Ebola outbreak in North Kivu is likely undercounted by as much as 50%, Oxfam warned Friday, citing a collapse in clean water access and sanitation infrastructure that has left communities vulnerable to undetected infections.
According to Oxfam’s emergency response team, the official toll of 130 confirmed cases since April—reported by the World Health Organization (WHO)—fails to account for unreported deaths in remote villages where testing remains scarce. “In some areas, we’re seeing families burying relatives with Ebola symptoms before they can even be tested,” said Oxfam’s East Africa director, Katrin Verkade, who visited affected regions last week. “This isn’t just a data gap; it’s a public health catastrophe waiting to happen.”
Why the numbers may be far worse
Oxfam’s assessment aligns with internal WHO estimates, obtained by Reuters earlier this month, suggesting the true case count could exceed 200. The discrepancy stems from three critical failures:
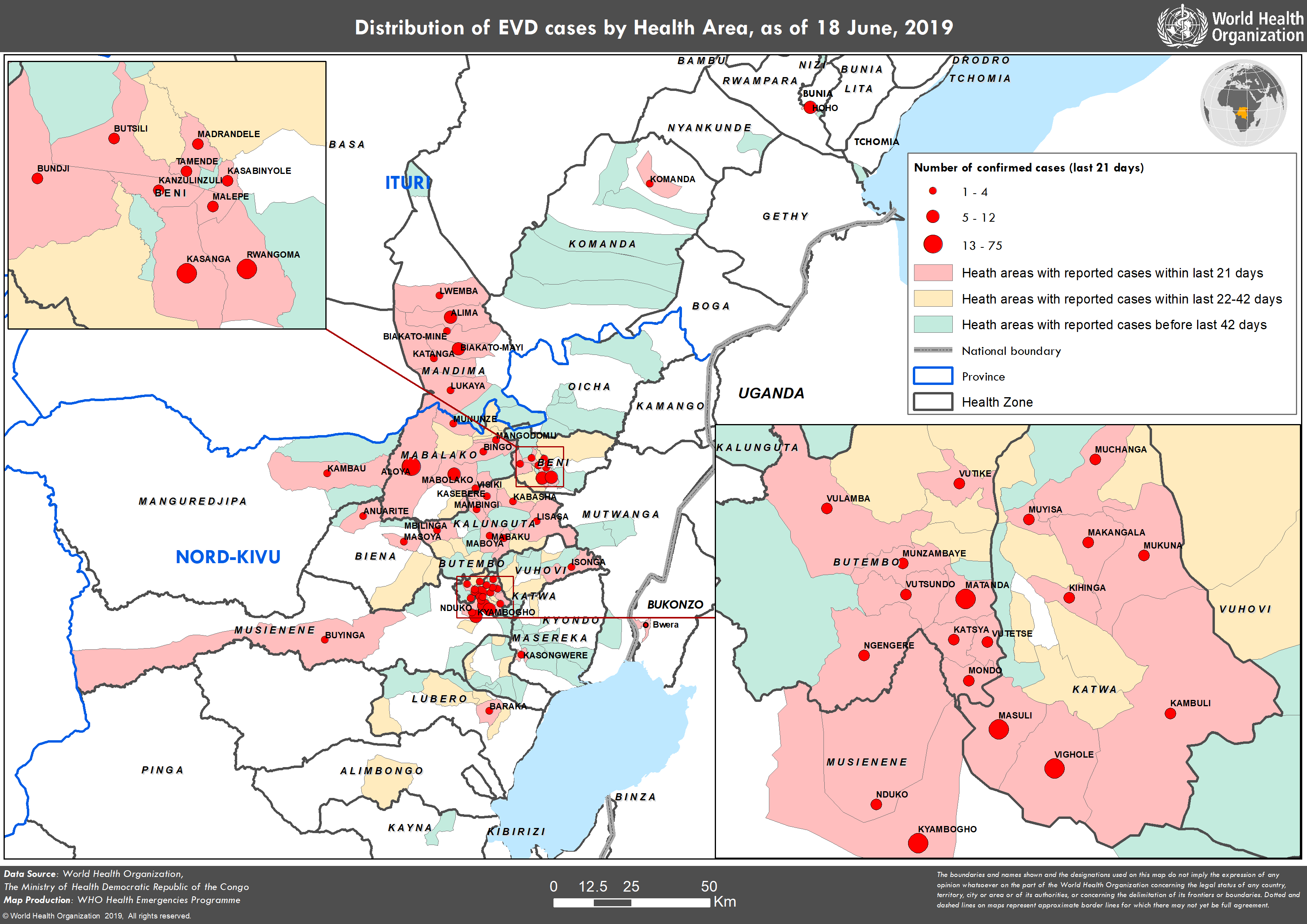
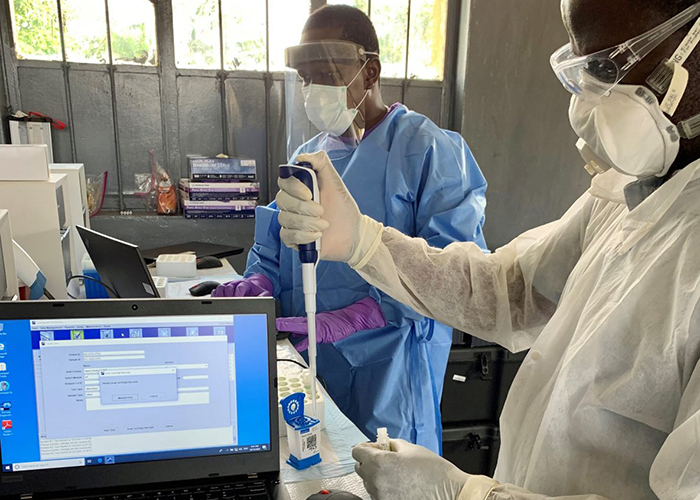
- Testing delays: Only 12 of 40 health zones in North Kivu have operational Ebola labs, forcing samples to be shipped to Goma—a journey that can take up to 48 hours. In the meantime, infected individuals spread the virus in households without running water.
- Sanitation collapse: A UNICEF report from June 10 found that 80% of households in Beni and Butembo lack access to soap or handwashing stations, violating WHO’s minimum hygiene standards for outbreak control.
- Distrust in authorities: Local leaders in some villages have blocked health workers after a WHO vaccination campaign in Mbandaka last year was linked to two deaths, though later investigations attributed those to unrelated causes. Oxfam documented three communities where families refused to report suspected cases.
How the outbreak compares to past epidemics
The current surge in North Kivu mirrors the 2018–2020 Eastern DRC outbreak, which became the second-deadliest in history after 2,280 deaths. That crisis was also plagued by underreporting, with WHO admitting in 2019 that only 40% of cases were ever confirmed. This time, however, the stakes are higher: North Kivu borders South Sudan and Uganda, raising fears of cross-border transmission.
“The difference now is the speed of movement,” said Dr. Michael Ryan, WHO’s executive director for emergencies, during a briefing in Geneva on Thursday. “In 2018, we had static hotspots. Today, we’re seeing Ebola spread along trucking routes and refugee paths—a recipe for regional spread.”
The Congolese government has deployed 1,200 additional troops to enforce quarantines, but Oxfam warns this risks further alienating communities already wary of state involvement. Meanwhile, the WHO’s $100 million emergency appeal remains 30% unfunded, leaving gaps in contact tracing and vaccination efforts.
What happens next: The UN’s divided response
The UN Security Council is scheduled to convene an emergency session on Monday to discuss whether to classify the outbreak as a “threat to international peace”—a designation that could unlock faster funding. However, Russia and China have already signaled resistance, citing concerns over “foreign interference in DRC sovereignty.”
In the meantime, Oxfam is pushing for a three-pronged solution:
- Mobile testing units in every health zone by July 15.
- Chlorination of water sources in high-risk areas, funded through the WHO’s $50 million sanitation reserve.
- A community-led burial protocol to reduce stigma around Ebola deaths.
The WHO’s Ebola Response Chief, Dr. Matshidiso Moeti, acknowledged the challenges in a statement Friday: “We’re not just racing against the virus; we’re racing against logistics and politics.” With no signs of the outbreak slowing, health workers on the ground describe the situation as “a perfect storm of failure.”