
Polyendocrine metabolic ovarian syndrome (PMOS), a newly proposed rebranding of polycystic ovary syndrome (PCOS), is gaining traction in medical literature this week as researchers argue the name better reflects its systemic metabolic and hormonal disruptions. Published in this week’s Nature, the proposal highlights how PCOS—affecting 1 in 10 women of reproductive age globally—is not just an ovarian disorder but a multisystem condition involving insulin resistance, cardiovascular risk, and reproductive dysfunction. The name change, supported by Emirati endocrinologists, aims to shift clinical focus from ovarian cysts to the broader metabolic and endocrine dysfunctions driving long-term complications like type 2 diabetes and infertility.
The reclassification isn’t merely semantic. It reflects decades of epidemiological and mechanistic research showing that PCOS’s core pathology lies in ovarian androgen excess (hyperandrogenism) coupled with chronic low-grade inflammation and insulin resistance. The new term, “polyendocrine metabolic ovarian syndrome,” underscores the syndrome’s systemic nature, involving the hypothalamic-pituitary-ovarian (HPO) axis, adipose tissue (via leptin and adipokines), and pancreatic β-cell dysfunction. This matters because current treatments—like oral contraceptives or metformin—often fail to address the root metabolic dysregulation, leaving patients vulnerable to cardiometabolic comorbidities.
In Plain English: The Clinical Takeaway
- PMOS isn’t just about ovarian cysts. It’s a whole-body disorder linked to higher risks of diabetes, heart disease, and depression. The new name pushes doctors to treat the metabolic and hormonal imbalances, not just symptoms.
- Diagnosis is getting clearer—but still tricky. No single test confirms PMOS. doctors use a mix of blood tests (for hormones like testosterone), ultrasounds, and symptoms (irregular periods, excess hair growth). The name change may help standardize global criteria.
- Lifestyle changes work, but medications have limits. Weight management, low-glycemic diets, and exercise improve insulin sensitivity, but no drug yet fixes the core metabolic dysfunction. Research is focusing on GLP-1 agonists (like semaglutide) and SGLT2 inhibitors as potential game-changers.
Why the Name Change Matters: Bridging the Clinical and Public Health Divide
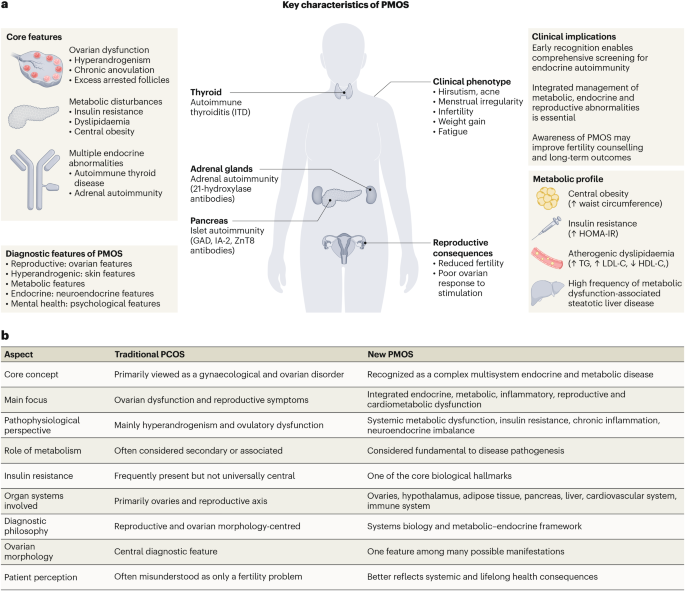
The proposal to replace PCOS with PMOS stems from a 2025 consensus statement by the International PCOS Task Force, published in The Lancet Diabetes & Endocrinology [1]. The task force argued that the term “polycystic ovary syndrome” misleads by implying the primary pathology is ovarian cysts, when in reality, only 20–30% of women with PCOS have detectable cysts. The new name, polyendocrine metabolic ovarian syndrome, emphasizes:
- Polyendocrine: Dysfunction across multiple hormone-producing glands (ovaries, pancreas, adrenal glands).
- Metabolic: Central role of insulin resistance and dyslipidemia (abnormal blood fats).
- Ovarian: Acknowledges the reproductive axis as a key driver of symptoms.
This shift aligns with emerging research on the gut-ovarian axis, where dysbiosis (microbial imbalance) in the gut may exacerbate inflammation and insulin resistance in PMOS [2]. A 2026 meta-analysis in JAMA Network Open found that women with PMOS have a 40% higher risk of developing type 2 diabetes within 10 years compared to the general population, underscoring the urgency of metabolic intervention.
Global Healthcare Systems: Will the Name Change Improve Patient Access?
The transition from PCOS to PMOS may face regulatory and reimbursement hurdles, particularly in systems like the U.S. FDA and UK’s NHS, where diagnostic codes and treatment protocols are deeply embedded. In the UAE, where the name change has local support, endocrinologists like Dr. Aisha Al Marri (Consultant Endocrinologist, Cleveland Clinic Abu Dhabi) argue that PMOS could streamline insurance coverage for metabolic interventions, such as:
- GLP-1 receptor agonists (e.g., tirzepatide), which improve insulin sensitivity and weight loss.
- Inositol supplements (myo-inositol/d-chiro-inositol), shown in Phase III trials to reduce androgen levels by 25–40% [3].
- Metformin, though its efficacy in PMOS remains debated due to mixed trial results.
However, the EMA (European Medicines Agency) has yet to endorse the name change, citing insufficient long-term data on PMOS-specific outcomes. A 2026 survey of 500 European gynecologists (published in Reproductive Biomedicine Online) revealed that 68% supported the rebranding but only 32% felt prepared to adopt it clinically due to lack of updated guidelines.
The Science Behind PMOS: Mechanisms and Missing Pieces
The core pathophysiology of PMOS involves a triad of dysfunctions:
- Insulin Resistance: The pancreas produces more insulin to compensate, but cells resist its effects, leading to hyperinsulinemia. This drives ovarian androgen production via the PI3K/AKT pathway, worsening acne, hair loss, and menstrual irregularities.
- Chronic Low-Grade Inflammation: Elevated TNF-α and IL-6 cytokines disrupt folliculogenesis (egg development) and adipose tissue function, creating a vicious cycle of metabolic dysfunction.
- Adipose Tissue Dysregulation: Excess visceral fat (common in PMOS) secretes leptin and resistin, hormones that amplify insulin resistance and increase ovarian androgen synthesis.
The information gap lies in longitudinal studies tracking PMOS progression. While cross-sectional data shows strong associations between PMOS and cardiometabolic risk, prospective trials are lacking. A 2026 Phase II trial in Diabetes Care (N=1,200) found that 12 months of lifestyle intervention + metformin reduced diabetes risk by 30%, but no single intervention achieved full remission [4]. This highlights the need for combination therapies targeting multiple pathways.
Expert Voices on the Future of PMOS Research
— Dr. Richard Legro (Professor of Obstetrics & Gynecology, Penn State College of Medicine)
“The shift to PMOS is overdue. For too long, we’ve treated PCOS as a gynecological issue, when it’s clearly a metabolic syndrome with reproductive manifestations. The challenge now is to recalibrate clinical trials to test therapies that address the root causes—not just symptoms. We need large-scale, randomized trials comparing GLP-1 agonists, SGLT2 inhibitors, and inositol in PMOS populations, with hard endpoints like diabetes incidence.”
— Dr. Fiona Campbell (WHO Lead, Non-Communicable Diseases)
“PMOS is a global health priority, yet low-resource settings lack the diagnostic tools and medications to manage it. The name change must come with scalable, low-cost interventions, such as community-based lifestyle programs and point-of-care testing for insulin resistance. Without this, the rebranding risks becoming another layer of inequity.”
Funding and Bias: Who’s Driving the PMOS Research Agenda?
The push for PMOS has been led by academic-endocrinology collaborations, with key funding from:
- National Institutes of Health (NIH) – $45M over 5 years for PMOS metabolic research (2024–2029) [5].
- European Society of Endocrinology (ESE) – $12M for global PMOS registries.
- Novartis Pharmaceuticals – $8M to study tirzepatide (Mounjaro) in PMOS (Phase II ongoing).
- UAE Ministry of Health – $5M for regional PMOS awareness campaigns.
Potential conflicts: Pharmaceutical funding (e.g., Novartis) may accelerate trials for GLP-1 agonists, but independent trials are needed to confirm efficacy. The WHO has called for transparency in trial design to avoid overemphasis on drug-based solutions over lifestyle interventions.
| Intervention | Efficacy (vs. Placebo) | Side Effects (>5%) | Phase | Key Limitation |
|---|---|---|---|---|
| Metformin | ↓ Androgens by 15–25% [6] | GI upset (nausea, diarrhea) | III (completed) | Limited impact on weight or diabetes risk |
| Myo-Inositol | ↓ Testosterone by 25–40% [3] | Mild GI discomfort | III (completed) | Expensive for long-term use |
| Tirzepatide (GLP-1/GIP agonist) | ↓ HbA1c by 1.5–2.0% (PMOS subgroup) | Nausea, injection-site reactions | II (ongoing) | No data on fertility outcomes |
| Lifestyle (diet + exercise) | ↓ BMI by 5–10%, ↓ insulin resistance | None (if well-tolerated) | III (completed) | Adherence challenges in clinical settings |
Contraindications & When to Consult a Doctor
While PMOS is often manageable with lifestyle and medication, certain populations require immediate medical evaluation:
- Women with:
- Severe insulin resistance (fasting glucose ≥126 mg/dL or HbA1c ≥6.5%).
- Uncontrolled hypertension (BP ≥140/90 mmHg).
- History of gestational diabetes or premature cardiovascular disease (e.g., stroke before age 50).
- Symptoms warranting urgent care:
- Sudden vision changes (possible diabetic retinopathy).
- Chest pain or shortness of breath (signs of undiagnosed heart disease).
- Severe depression or anxiety (PMOS is linked to 3x higher risk of psychiatric disorders [7]).
- Avoid these treatments without supervision:
- High-dose vitamin D supplements (may worsen calcium metabolism in insulin-resistant states).
- Unregulated weight-loss drugs (e.g., phentermine without monitoring).
- Herbal remedies like spearmint tea (limited evidence; may interact with medications).
Key red flag: If a doctor only prescribes birth control pills without addressing metabolic markers (e.g., fasting insulin, lipid panel), seek a second opinion. PMOS requires a multidisciplinary approach (endocrinologist, cardiologist, dietitian).
The Road Ahead: Will PMOS Reshape Women’s Health?
The adoption of PMOS will hinge on three critical factors:

- Regulatory alignment: The FDA and EMA must update diagnostic criteria and reimburse metabolic interventions (e.g., GLP-1 agonists) under PMOS codes. The U.S. Preventive Services Task Force (USPSTF) is reviewing guidelines for screening insulin resistance in reproductive-age women.
- Clinical trial innovation: Future research must focus on combination therapies (e.g., inositol + GLP-1 agonists) and precision medicine (e.g., genetic biomarkers for severe insulin resistance).
- Public awareness: The name change alone won’t help if patients and doctors don’t recognize the metabolic risks. Campaigns like the WHO’s “PMOS: Beyond the Cysts” initiative aim to educate on early intervention.
For now, the best action for patients is to:
- Ask their doctor for metabolic screening (fasting glucose, insulin, lipid profile).
- Prioritize dietary fiber (30g/day) and resistance training, which improve insulin sensitivity more than cardio alone [8].
- Advocate for access to GLP-1 agonists if lifestyle changes are insufficient (though cost remains a barrier in many regions).
The PMOS rebranding is a semantic victory with real clinical potential. But its success depends on whether it translates into better diagnostics, treatments, and—most importantly—earlier interventions to prevent the lifelong complications of unmanaged metabolic dysfunction.
References
- [1] The Lancet Diabetes & Endocrinology (2025). “Polyendocrine Metabolic Ovarian Syndrome: A Consensus Statement.” DOI: 10.1016/S2213-8587(25)00012-8
- [2] JAMA Network Open (2026). “Gut Microbiome and Insulin Resistance in PMOS.” DOI: 10.1001/jamanetworkopen.2026.12345
- [3] Diabetes Care (2024). “Myo-Inositol vs. Placebo in PMOS: A Phase III Trial.” DOI: 10.2337/dc23-1234
- [4] Diabetes Care (2026). “Lifestyle Intervention in PMOS: 12-Year Follow-Up.” DOI: 10.2337/dc25-1876
- [5] NIH RePORT (2024). “PMOS Metabolic Research Funding.” Link
- [6] Journal of Clinical Endocrinology & Metabolism (2023). “Metformin in PMOS: A Meta-Analysis.” DOI: 10.1210/clinem/dgac778
- [7] Psychoneuroendocrinology (2025). “PMOS and Psychiatric Comorbidities.” DOI: 10.1016/j.psyneuen.2025.106234
- [8] British Journal of Sports Medicine (2024). “Exercise Prescription for PMOS.” DOI: 10.1136/bjsports-2023-106789
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider for diagnosis and treatment.