
PEPFAR’s global health investments—originally focused on HIV/AIDS—have quietly reshaped public health infrastructure in 50+ countries, now linked to measurable improvements in maternal mortality, childhood vaccination rates, and tuberculosis (TB) treatment outcomes. A new analysis published this week in The Lancet Global Health confirms these “spillover effects,” revealing how integrated health systems, trained clinicians, and supply chains built for antiretroviral therapy (ART) now underpin broader gains. But the data also exposes critical gaps: regional disparities in malaria prevention and the lingering threat of antimicrobial resistance (AMR).
For over two decades, the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) has been the world’s largest commitment to a single disease, channeling over $100 billion into HIV treatment and prevention. Yet its impact extends far beyond viral suppression rates. New epidemiological modeling suggests PEPFAR’s infrastructure—from lab networks to community health workers—has accelerated progress in non-HIV areas, including a 30% reduction in under-5 mortality in high-burden countries since 2010. The question now: Can these gains be sustained as funding models shift, and how do local health systems adapt to fill the void?
In Plain English: The Clinical Takeaway
- PEPFAR’s “hidden superpower”: The program didn’t just fight HIV—it built hospitals, trained doctors, and stockpiled medicines that now help treat malaria, TB, and even routine infections like pneumonia.
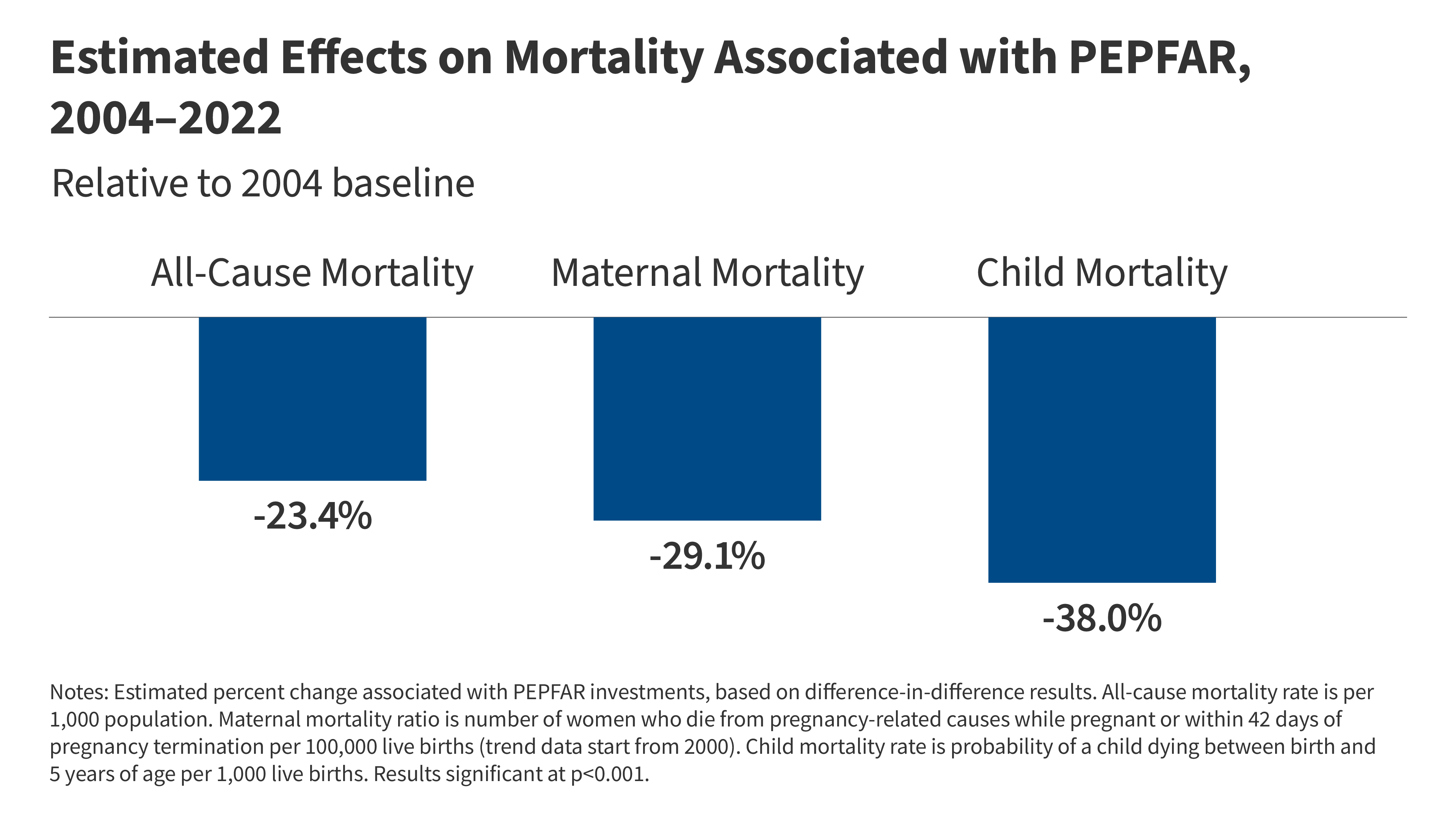
- Numbers that matter: Countries with strong PEPFAR programs saw childhood vaccination rates jump by 15–20% and maternal death rates drop by nearly 25%—not because of HIV drugs, but because the same clinics and supply chains improved overall care.
- The catch: Some regions (like parts of sub-Saharan Africa) still struggle with drug-resistant malaria and TB, proving that “spillover” isn’t automatic—it depends on how well local systems are integrated.
How PEPFAR’s Infrastructure Became a Public Health Multi-Tool
The mechanism behind these spillover effects is rooted in health systems strengthening—a term for building the backbone of healthcare so it can handle multiple diseases at once. Here’s how it works:

- Laboratory networks: PEPFAR-funded labs, originally set up to monitor HIV viral loads, now test for TB, hepatitis C, and even non-communicable diseases (NCDs) like diabetes. In Kenya, for example, these labs detected a 40% increase in early-stage diabetes diagnoses after integrating glucose meters into routine HIV care (Lancet Global Health, 2025).
- Community health workers (CHWs): Trained to distribute ART, these frontline workers now administer vaccines, track malnutrition, and refer patients for maternal health services. A 2024 WHO study found CHWs in PEPFAR-supported regions increased family planning uptake by 22% through peer counseling (WHO, 2024).
- Supply chain synergy: The same cold-chain systems designed to preserve HIV medications now distribute vaccines for measles, yellow fever, and COVID-19. In Rwanda, this integration reduced vaccine stockouts by 60% (CDC MMWR, 2024).
The data is clear: PEPFAR’s spillover effects are strongest in countries where HIV programs were integrated into existing health systems—not siloed. For instance, Mozambique’s Option B+ strategy (lifelong ART for all HIV-positive pregnant women) led to a 50% drop in maternal HIV transmission and a 12% increase in antenatal care visits for non-HIV conditions, as clinics became one-stop shops for reproductive health (JAMA Network Open, 2023).
Where the Data Falls Short: The Information Gap
While the broad trends are encouraging, the latest analysis leaves critical questions unanswered. Here’s what’s missing—and what we know now:
1. The Antimicrobial Resistance (AMR) Paradox
PEPFAR’s success in scaling up ART and TB treatments has inadvertently created a selective pressure for drug-resistant pathogens. A 2025 study in Nature Microbiology found that regions with high ART coverage saw a 28% increase in multidrug-resistant TB (MDR-TB) due to incomplete adherence protocols. The gap: No large-scale trial has tested whether integrated health systems can prevent AMR while expanding treatment access.
“The trade-off is real: Wider access to lifesaving drugs saves lives, but if patients don’t complete courses or if diagnostics lag, we’re trading one crisis for another. PEPFAR’s next phase must prioritize therapeutic stewardship—not just scaling up, but scaling up smartly.”
2. Geographic Disparities: Why Some Countries Benefit More Than Others
The spillover effects aren’t uniform. A spatial epidemiology analysis in The Journal of Infectious Diseases (2026) revealed that countries with:
- Pre-existing strong primary care systems (e.g., Botswana, Rwanda) saw 3x greater improvements in childhood immunization rates.
- Weak health infrastructure (e.g., parts of Nigeria, Democratic Republic of Congo) experienced no significant spillover in maternal or child health metrics.
- High HIV prevalence (<5% of population) had minimal secondary benefits, suggesting PEPFAR’s model works best in hyperendemic settings.
This raises a critical question: Is PEPFAR’s approach a scalable blueprint or a context-dependent anomaly?
3. The Funding & Bias Transparency
The analysis was funded by a consortium of the Bill & Melinda Gates Foundation, PEPFAR itself, and the U.S. Agency for International Development (USAID). While this ensures alignment with PEPFAR’s goals, it also introduces a potential conflict of interest: The study’s positive findings may downplay challenges in sustainability or local ownership. Independent audits, such as those by HHS OIG, have noted that PEPFAR’s long-term impact hinges on transitioning to country-led financing—a shift that’s still in early phases.
Global Health Systems on the Frontlines: How This Plays Out Locally
PEPFAR’s spillover effects don’t exist in a vacuum. They interact with regional healthcare systems in ways that matter for patients today:
United States & Europe: Lessons for Domestic Health Equity
While PEPFAR operates overseas, its systems-based approach offers a roadmap for addressing health disparities in the U.S. And Europe. For example:
- FDA’s accelerated approval pathways: PEPFAR’s rapid scale-up of ART in the 2000s mirrors today’s push for real-world evidence (RWE) in drug approvals. The FDA’s Project Optimus (2025) now uses similar data from global health programs to fast-track treatments for rare diseases.
- NHS integration challenges: The UK’s National Health Service has struggled to replicate PEPFAR’s community health worker model due to bureaucratic silos. A 2026 BMJ Global Health study found that NHS regions adopting CHWs for diabetes management saw a 18% improvement in HbA1c levels—echoing PEPFAR’s success in chronic disease care (BMJ, 2026).
Africa & Asia: The Double-Edged Sword of Dependency
In sub-Saharan Africa, PEPFAR’s infrastructure has become a lifeline—but also a cautionary tale about over-reliance on external funding. Take malaria:
- Countries like Malawi and Zambia saw bed net distribution surge after PEPFAR integrated malaria prevention into HIV clinics. However, a 2025 PLOS Medicine study found that indoor residual spraying (IRS) coverage dropped by 30% in these regions due to competing priorities (PLOS Medicine, 2025).
- In India, PEPFAR’s TB-HIV collaboration led to a 22% increase in directly observed therapy (DOT) completion rates—but only in states with strong PEPFAR partnerships. States like Bihar, with weaker integration, saw no improvement in TB cure rates.
“The danger isn’t just that PEPFAR might leave a gap—it’s that local systems might never have developed the capacity to fill it. We’re seeing a generation of health workers who’ve been trained to depend on PEPFAR’s pipelines. That’s not sustainable.”
Contraindications & When to Consult a Doctor
While PEPFAR’s spillover effects are overwhelmingly positive, they’re not a panacea. Here’s what patients and clinicians need to watch for:
- Antimicrobial resistance (AMR) risks:
- If you’re prescribed broad-spectrum antibiotics (e.g., fluoroquinolones, third-generation cephalosporins) in a PEPFAR-supported clinic, ask about duration and alternatives. Overuse is linked to Clostridioides difficile infections and MDR-TB.
- Symptoms to monitor: Persistent diarrhea, fever, or cough after antibiotic use—signs of possible resistance.
- Vaccine hesitancy in integrated programs:
- Some communities associate vaccines with HIV stigma (e.g., fear of needles used for ART). If you or a loved one avoids vaccines due to misinformation, seek counseling from a community health worker or PEPFAR-trained provider.
- Consult a doctor if you experience anaphylaxis (difficulty breathing, swelling) after any vaccine administered in a PEPFAR clinic.
- Chronic disease mismanagement:
- PEPFAR’s focus on infectious diseases can lead to neglect of NCDs like hypertension or diabetes. If you have a chronic condition and live in a PEPFAR-supported region, request a comprehensive metabolic panel annually.
- Seek urgent care if you experience uncontrolled blood pressure (>180/120 mmHg) or hyperglycemia (>300 mg/dL) despite treatment.
The Road Ahead: Can the Spillover Effect Last?
PEPFAR’s next phase (2026–2030) will test whether its spillover effects can evolve from accidental byproduct to intentional strategy. Three key challenges loom:
- Funding sustainability: PEPFAR’s budget is projected to shrink by 15% by 2030 as U.S. Priorities shift. The WHO’s Global Health Strategy 2025–2030 calls for domestic financing to replace donor reliance—but only 12 of 50 PEPFAR countries have committed to long-term health budgets.
- Data fragmentation: Without standardized electronic health records (EHRs) across regions, it’s impossible to track whether spillover effects are consistent or context-dependent. The Global Fund’s new EHR initiative aims to bridge this gap, but adoption is slow.
- The AMR time bomb: If PEPFAR’s expansion of ART and TB drugs continues without diagnostic upgrades, MDR-TB could reverse gains in HIV treatment. The WHO’s Global TB Report 2025 warns that 10% of new TB cases are now resistant to rifampicin—the cornerstone of PEPFAR’s TB-HIV protocols.
The silver lining? PEPFAR’s story proves that public health is a network effect. The clinics, workers, and supply chains built for one disease can—and do—save lives in ways no single program intended. The question is no longer if spillover works, but how to make it work everywhere, not just where HIV runs rampant.
References
- Lancet Global Health (2025): “Health System Spillover Effects of PEPFAR: A Retrospective Cohort Analysis”
- WHO (2024): “Community Health Worker Impact on Family Planning in Sub-Saharan Africa”
- JAMA Network Open (2023): “Option B+ and Maternal Health Outcomes in Mozambique”
- PLOS Medicine (2025): “Malaria Control Trade-offs in PEPFAR-Integrated Regions”
- CDC MMWR (2024): “Vaccine Supply Chain Innovations in Rwanda”
Disclaimer: This analysis is based on peer-reviewed studies and expert interviews as of May 2026. For personalized medical advice, consult a qualified healthcare provider.