
Premenstrual Dysphoric Disorder (PMDD) is a severe, clinical manifestation of premenstrual syndrome (PMS) that significantly impairs daily functioning. Activists in the Netherlands are currently completing a 60-kilometer walk to increase public awareness of this neuroendocrine condition, which affects approximately 3% to 8% of menstruating individuals globally, often leading to significant diagnostic delays.
In Plain English: The Clinical Takeaway
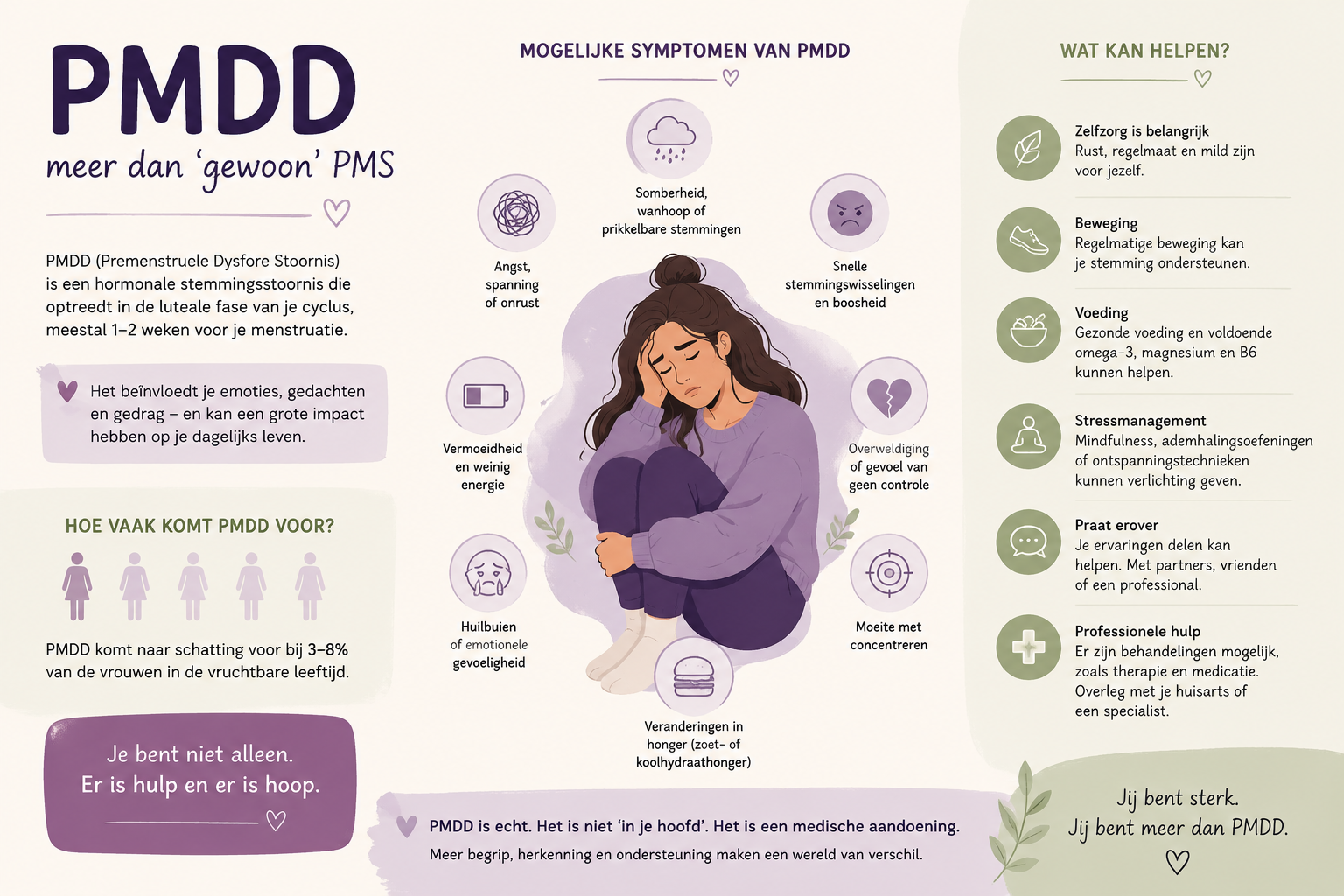
- Not Just PMS: Unlike PMS, which involves mild physical or mood symptoms, PMDD is a formal psychiatric diagnosis characterized by debilitating emotional instability, anxiety, and depression linked specifically to the luteal phase of the menstrual cycle.
- Biological Basis: PMDD is not a “hormonal imbalance” in the traditional sense; rather, it is an abnormal neurobiological sensitivity to the normal fluctuations of progesterone metabolites, specifically allopregnanolone, which impacts GABA-A receptor function in the brain.
- Diagnostic Gold Standard: Clinical guidelines require the prospective tracking of symptoms over at least two menstrual cycles to differentiate PMDD from underlying mood disorders like Major Depressive Disorder (MDD) or Generalized Anxiety Disorder (GAD).
The Neurobiological Mechanism of PMDD
The pathophysiology of PMDD is rooted in how the brain responds to reproductive steroids. According to the National Institutes of Health (NIH), individuals with PMDD exhibit a unique sensitivity to allopregnanolone, a metabolite of progesterone. In most individuals, this metabolite acts as a neurosteroid that promotes calmness. In those with PMDD, however, the GABA-A receptors—the brain’s primary inhibitory signaling system—fail to respond appropriately to these changes during the luteal phase.

“The diagnostic challenge remains significant because PMDD is often misdiagnosed as bipolar disorder or clinical depression. The definitive marker is the remission of symptoms within days of the onset of menses,” notes Dr. Tory Eisenlohr-Moul, a leading researcher in reproductive psychiatry.
This neurobiological divergence explains why standard serotonin-based antidepressants, such as Selective Serotonin Reuptake Inhibitors (SSRIs), are highly effective for PMDD even when taken only during the luteal phase. This “intermittent dosing” strategy is a unique pharmacological approach rarely seen in other psychiatric conditions, reflecting the cycle-specific nature of the disorder.
Diagnostic Criteria and Epidemiological Data
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) classifies PMDD under Depressive Disorders. To meet the clinical threshold, a patient must report at least five symptoms, including affective lability (mood swings), irritability, or depressed mood, that occur in the week before menses and resolve shortly after. The following table illustrates the clinical distinction between PMS and PMDD.

| Feature | PMS | PMDD |
|---|---|---|
| Symptom Severity | Mild to moderate | Severe and debilitating |
| Functional Impact | Minimal | High (work/social impairment) |
| Primary Symptoms | Physical (bloating, breast tenderness) | Affective (rage, suicidal ideation, anxiety) |
| Diagnostic Basis | Clinical presentation | Prospective daily rating scales |
Regulatory Landscapes and Patient Access
In Europe, the European Medicines Agency (EMA) provides guidelines for the management of severe menstrual disorders, yet access to specialized care remains fragmented. In the Netherlands, as highlighted by current advocacy efforts, the gap between symptom onset and formal diagnosis frequently spans over a decade. This delay is often attributed to the historical trivialization of women’s reproductive health and the lack of standardized screening tools in primary care settings.
For patients, the path to treatment often involves navigating a complex web of gynecological and psychiatric care. While the FDA in the United States has approved specific SSRIs for PMDD, such as fluoxetine and sertraline, off-label use of combined oral contraceptives is common practice across the EU to suppress ovulation entirely, thereby eliminating the hormonal trigger for the symptoms.
Contraindications & When to Consult a Doctor
Patients experiencing symptoms that interfere with work, education, or relationships should consult a primary care physician or a gynecologist. Intervention is critical if symptoms include suicidal ideation or severe panic attacks.
Contraindications: Hormonal therapies, such as oral contraceptives, are contraindicated in patients with a history of venous thromboembolism (blood clots), uncontrolled hypertension, or estrogen-sensitive cancers. SSRIs should be used with caution in patients with a history of manic episodes, as they may trigger a shift into bipolar disorder. Always disclose all current medications to a provider to avoid serotonin syndrome, a potentially life-threatening condition caused by excessive serotonin accumulation.
The Future of PMDD Research
Current research efforts are shifting toward identifying genetic markers that predispose individuals to this neurosteroid sensitivity. Funding for such studies, often supported by organizations like the International Association for Premenstrual Disorders (IAPMD), is essential to moving beyond symptom management and toward targeted molecular therapies. As advocacy groups continue to push for greater visibility, the medical community is gradually moving toward a more standardized, evidence-based approach to this reproductive health crisis.
