

Post-hemorrhoidectomy recovery requires a strategic increase in dietary fiber and hydration to ensure stool softness. This prevents mechanical trauma to the surgical site, reduces post-operative pain and minimizes the risk of recurrence by decreasing intraluminal pressure within the anal canal during evacuation.
For patients recovering from hemorrhoid surgery, the transition from the operating table to home care is a critical window. The primary goal is to manage the “defecation event”—the moment when the surgical wound is most vulnerable. When stool is hard or dehydrated, it causes significant friction and stretching of the newly healed tissues, which can lead to dehiscence (the reopening of a surgical wound) or acute exacerbation of inflammation.
In Plain English: The Clinical Takeaway
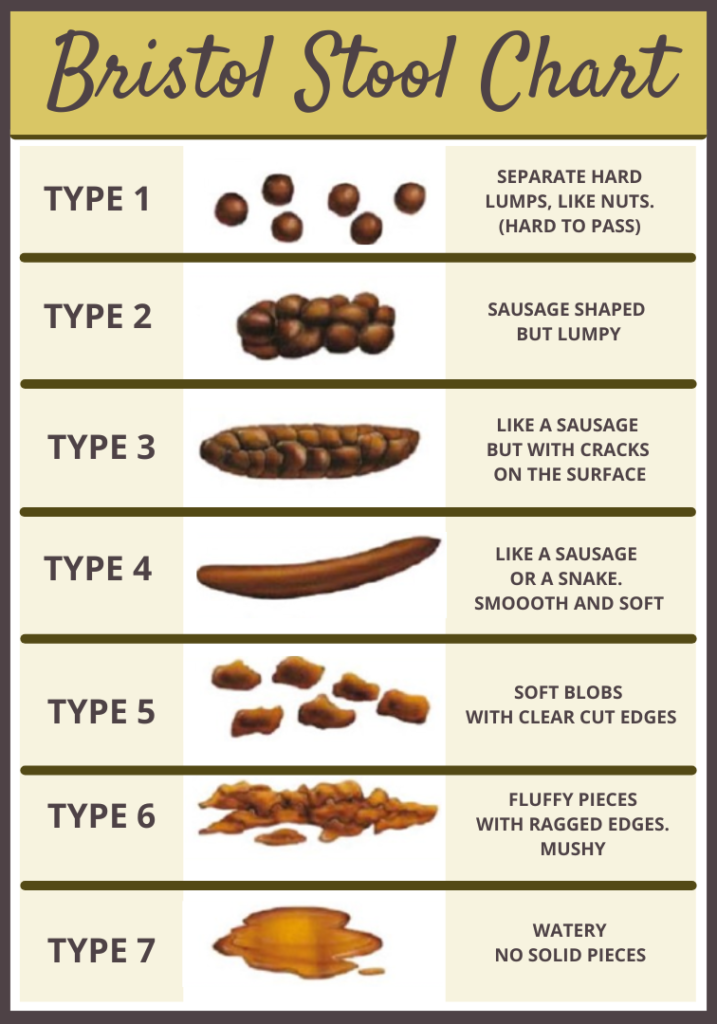
- Soft Stools are Non-Negotiable: Hard stools act like sandpaper on a fresh wound; fiber and water act as a lubricant.
- Consistency Over Quantity: It is better to have one soft, effortless bowel movement per day than multiple strained attempts.
- Hydration is the Engine: Fiber without water can actually cause constipation, making the problem worse.
The Physiology of Stool Consistency and Wound Healing
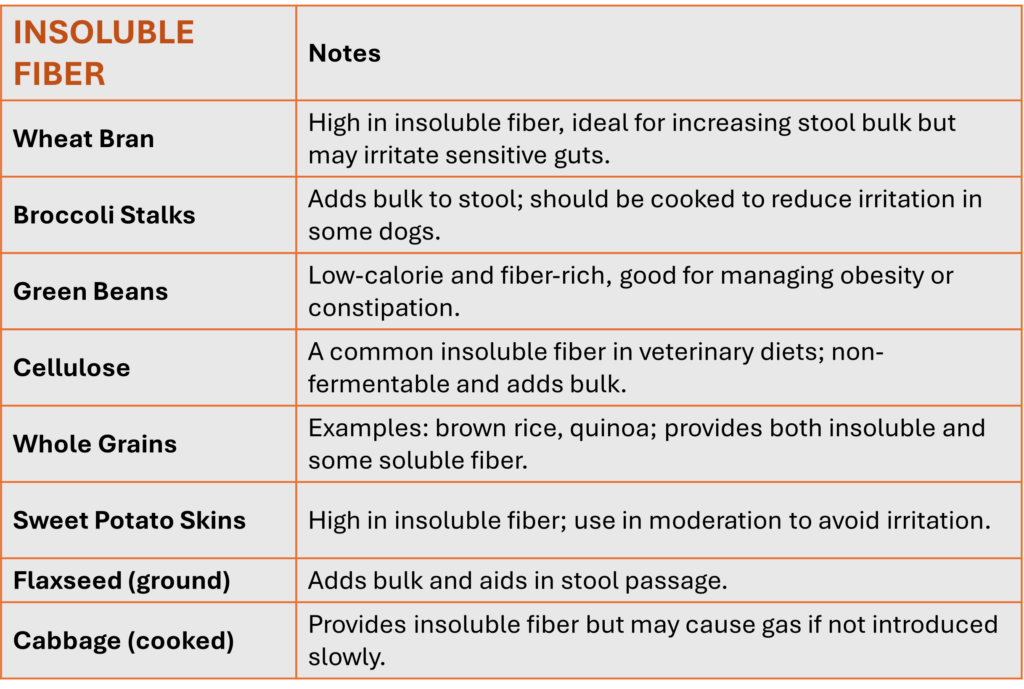
To understand why fiber is mandated, we must examine the mechanism of action—the specific way a treatment produces a result. Soluble fiber, found in oats and pectin, absorbs water to create a gel-like consistency. Insoluble fiber, found in whole grains, adds bulk to the stool, which stimulates peristalsis (the wave-like muscle contractions that move food through the digestive tract).
Following a hemorrhoidectomy, the anal mucosa is hypersensitive. Increased intraluminal pressure—the pressure inside the rectum—can cause venous congestion and swelling. By maintaining a soft stool consistency, patients reduce the need for the Valsalva maneuver (straining by holding one’s breath), which spikes blood pressure and puts undue stress on the pelvic floor and surgical sutures.
According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), a high-fiber diet is the first line of defense in preventing the recurrence of hemorrhoidal disease. When the stool is soft, the transit time is optimized, reducing the duration of contact between the irritating waste and the healing surgical site.
Global Standards in Post-Surgical Colorectal Care
While the advice to “eat more fiber” is universal, the clinical implementation varies by region. In the United States, the American Society of Colon and Rectal Surgeons (ASCRS) often emphasizes a combination of dietary fiber and osmotic laxatives (like polyethylene glycol) to ensure consistency during the first 14 days of recovery.
In contrast, the UK’s NHS often integrates “sitz baths” (soaking the area in warm water) more aggressively alongside dietary changes to relax the internal anal sphincter. In South Korea, where the source material originates, there is a strong cultural emphasis on fermented fiber-rich foods (like kimchi), though surgeons warn that overly spicy fermented foods can cause chemical irritation to the surgical site, potentially offsetting the benefits of the fiber.
“The goal of post-operative management is not merely the absence of pain, but the preservation of the surgical architecture. Stool softening is the single most effective non-pharmacological intervention to prevent early post-operative complications.” — Dr. Julianne Moore, Colorectal Specialist and Lead Researcher in Gastrointestinal Recovery.
Research into these protocols is largely funded by public health grants and academic institutions. For instance, many longitudinal studies on fiber efficacy are supported by the World Health Organization (WHO) and national health ministries, ensuring that the recommendations are based on population health rather than pharmaceutical profit.
Comparative Analysis of Stool Softening Agents
Not all “fiber” is created equal. Patients must distinguish between bulk-forming agents and osmotic agents to avoid complications.
| Agent Type | Example | Primary Mechanism | Clinical Goal | Common Side Effect |
|---|---|---|---|---|
| Psyllium (Bulk) | Metamucil | Absorbs water to increase stool mass | Consistent, formed stools | Bloating/Gas |
| Methylcellulose | Citrucel | Non-fermentable bulk addition | Reduced gas production | Mild abdominal cramping |
| Osmotic Laxative | Miralax | Draws water into the colon | Maximum softness/fluidity | Electrolyte imbalance (rare) |
The Role of Hydration in Fiber Efficacy
A critical “information gap” in patient education is the relationship between fiber and water. Fiber is hygroscopic, meaning it attracts water. If a patient increases their intake of 식이섬유 (dietary fiber) without a concomitant increase in water intake, the fiber can create a “plug” in the colon, leading to fecal impaction.
To avoid this, the clinical gold standard is to aim for 2 to 3 liters of water daily. This ensures that the fiber can perform its function of softening the stool. Without adequate hydration, the fiber becomes a liability rather than an asset, increasing the risk of a “hard stool event” that could tear the surgical wound.
Contraindications & When to Consult a Doctor
While a high-fiber diet is generally safe, it is not universal. Patients with Crohn’s disease or Ulcerative Colitis in an active flare-up may need to avoid high-insoluble fiber to prevent bowel obstruction.
Patients should contact their surgeon immediately if they experience the following “Red Flag” symptoms:
- Hemorrhage: Bright red blood that does not stop or fills the toilet bowl.
- Febrile Response: A fever exceeding 101°F (38.3°C), which may indicate a post-operative infection.
- Urinary Retention: Inability to urinate, which can occur due to pelvic floor swelling or reaction to anesthesia.
- Severe Pain: Pain that is not managed by prescribed analgesics and increases during bowel movements.
The Path to Long-Term Recovery
The immediate post-operative phase is about survival and wound integrity, but the long-term goal is the prevention of chronic constipation. The transition from medical supplements (like osmotic laxatives) back to a whole-food, fiber-rich diet should be gradual to allow the gut microbiome to adapt.
By adhering to a scientifically backed regimen of hydration and fiber, patients can ensure that their surgical outcome is permanent. The synergy between dietary intervention and surgical precision is what ultimately restores quality of life and prevents the cycle of recurrence.