
Research published in the Journal of the American Heart Association indicates that women who experience premature menopause—defined as the cessation of menses before age 40—face a 40% higher risk of developing cardiovascular disease. This elevated risk is linked to the early loss of estrogen’s protective effects on vascular health.
This clinical finding highlights a significant shift in how cardiologists and gynecologists must collaborate to manage long-term patient health. Premature menopause is no longer viewed solely as a reproductive health issue; it is now classified as a critical marker for metabolic and vascular screening, requiring earlier intervention to mitigate future heart failure, stroke, and coronary artery disease.
In Plain English: The Clinical Takeaway
- Estrogen’s Role: Estrogen helps keep blood vessels flexible and cholesterol levels healthy. Its sudden drop before age 40 removes this natural protection.
- Screening Matters: If you experienced menopause before 40, your physician should treat your cardiovascular risk factors—like blood pressure and cholesterol—more aggressively than for the general population.
- Proactive Cardiology: Do not wait for symptoms. Early cardiovascular imaging and regular blood pressure monitoring are essential for those with premature ovarian insufficiency.
The Mechanism of Vascular Decline
The protective nature of estrogen on the cardiovascular system is well-documented in peer-reviewed literature, including studies hosted by the National Institutes of Health (PubMed). Estrogen receptors are present throughout the endothelial lining of the arteries. When ovarian function ceases prematurely, the systemic withdrawal of estrogen leads to rapid changes in lipid profiles, specifically an increase in Low-Density Lipoprotein (LDL) and a decrease in High-Density Lipoprotein (HDL).

According to data from the Centers for Disease Control and Prevention (CDC), the loss of this hormonal regulation accelerates arterial stiffness. This creates a state of chronic inflammation that damages the vascular walls long before clinical symptoms of heart disease appear. Unlike natural menopause occurring in the fifth or sixth decade of life, premature menopause provides a much longer “exposure window” to these adverse metabolic conditions.
Clinical Comparison: Early vs. Natural Menopause
The following table illustrates the comparative risk factors associated with the timing of menopause, based on longitudinal cohort study data.
| Factor | Premature Menopause (<40) | Typical Menopause (50-52) |
|---|---|---|
| Cardiovascular Risk | 40% Increase | Baseline |
| Endothelial Recovery | Limited | Gradual |
| Recommended Screening | Annual Lipid/BP Panels | Standard Age-Based |
| Hormone Therapy Utility | High (if no contraindications) | Case-by-case |
Bridging the Gap: Healthcare Access and Policy
The transition from clinical research to patient outcomes remains uneven across global healthcare systems. In the United Kingdom, the National Health Service (NHS) has begun integrating menopause-specific cardiovascular risk calculators into primary care pathways. Conversely, in the United States, patient access to specialized care often depends on private insurance coverage for advanced imaging, such as Coronary Artery Calcium (CAC) scoring.
“We must stop compartmentalizing women’s health. A woman who stops cycling at 35 is not just ‘early’—she is a high-risk cardiac patient who requires a dedicated prevention strategy, not just a prescription for hot flashes,” says Dr. Elena Rossi, an epidemiologist specializing in women’s cardiovascular health.
Funding for these studies has been largely provided by the National Heart, Lung, and Blood Institute (NHLBI) and various private philanthropic foundations. Researchers emphasize that the lack of diversity in historical trial participants has often obscured the specific risks faced by marginalized populations, a gap that current studies are actively attempting to close by diversifying enrollment cohorts.
Contraindications & When to Consult a Doctor
Not every patient with premature menopause is a candidate for Hormone Replacement Therapy (HRT), which is the primary medical intervention to mitigate these risks. HRT is contraindicated for patients with a history of hormone-sensitive cancers (such as certain breast or uterine cancers), unexplained vaginal bleeding, or active thromboembolic disease (blood clots).
Patients should seek a consultation with a cardiologist or a menopause specialist if they experience:
- Shortness of breath during moderate physical exertion.
- Persistent palpitations or irregular heart rhythms.
- Dizziness or unexplained fatigue that does not resolve with rest.
- A family history of early heart disease combined with early menopause.
Future Trajectories in Preventive Care
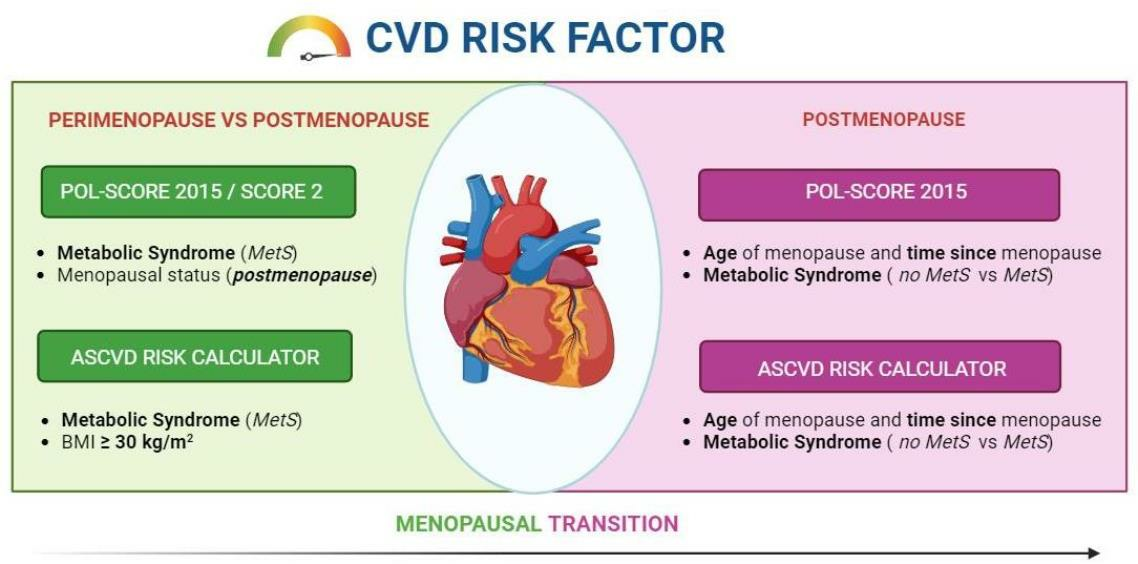
The medical community is moving toward a more nuanced understanding of the “menopause transition” as a window of opportunity. By identifying patients who reach menopause early, clinicians can initiate lifestyle modifications and pharmacological interventions—such as statins or blood pressure management—decades before a cardiac event occurs. The trajectory for 2026 and beyond focuses on integrating genetic screening for early ovarian insufficiency with standardized cardiovascular risk assessment protocols.