
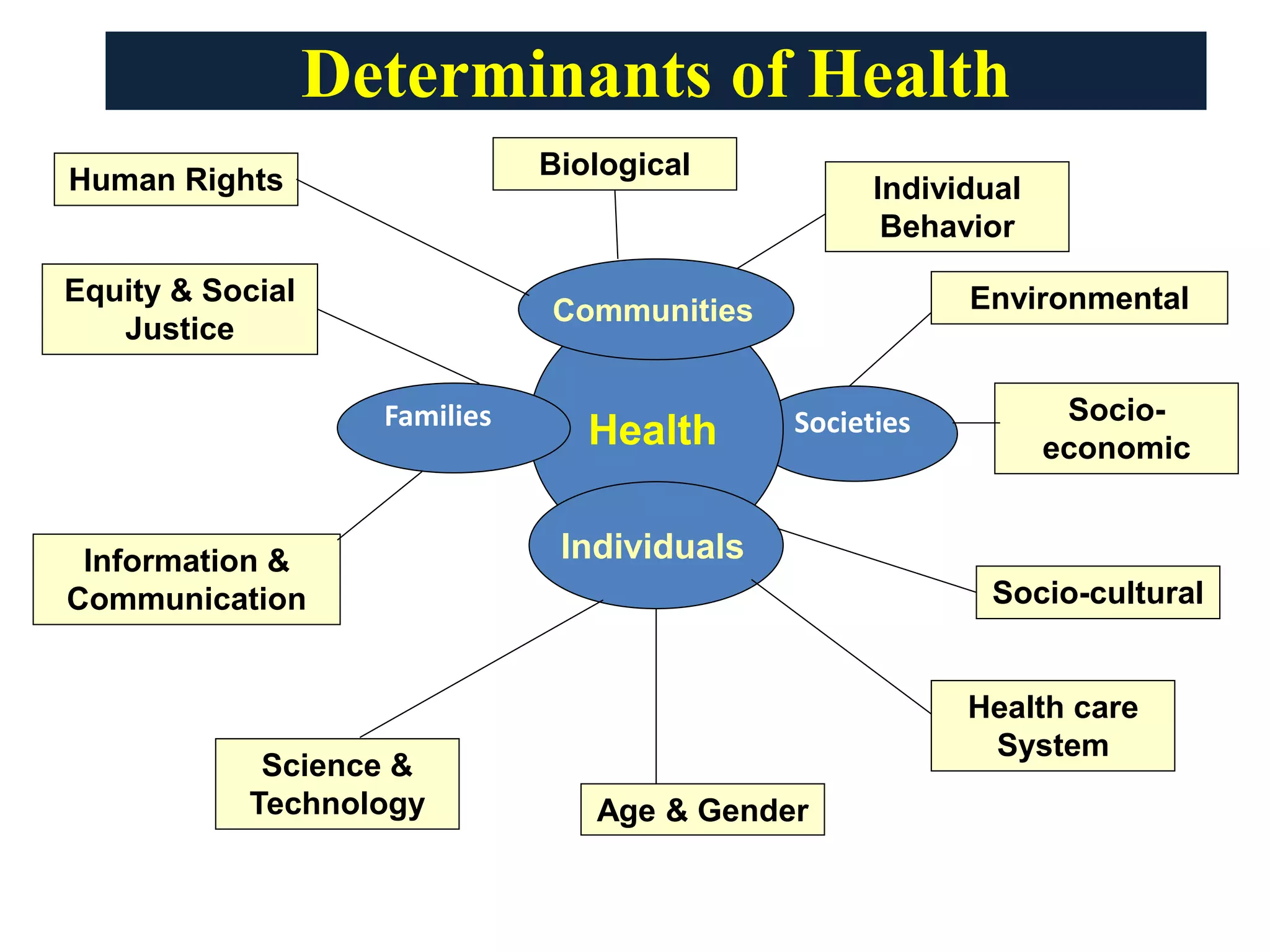
Access to quality health information is now recognized as a fundamental determinant of health. A new analysis published this week in Nature Medicine reveals that health literacy—the ability to find, understand and use medical information—directly correlates with clinical outcomes, reducing preventable hospitalizations and bridging systemic gaps in global health equity.
For decades, the medical community focused on the “Social Determinants of Health” (SDOH)—factors like socioeconomic status, neighborhood safety, and food security. However, we are now seeing that information is the catalyst that activates all other determinants. A patient may have access to a world-class clinic and the latest pharmaceuticals, but if they cannot synthesize the instructions for a complex medication regimen or understand the warning signs of a post-surgical infection, the clinical intervention is functionally neutralized.
In Plain English: The Clinical Takeaway
- Health Literacy is a Life-Saver: Being able to understand medical advice is just as important as the medicine itself; poor understanding leads to higher rates of emergency room visits.
- Information Equity: Quality health data should not be a luxury. Whether you are in a rural village or a major city, the “truth” about your health should be accessible and easy to understand.
- The “Infodemic” Risk: In an era of social media, the ability to distinguish evidence-based medicine from “wellness” myths is a critical survival skill.
The Pathophysiology of the Information Gap
The gap in health information creates a measurable clinical pathology. When patients experience low health literacy, they suffer from increased “cognitive load”—the mental effort required to process complex information. In high-stress clinical environments, this load often leads to “decisional paralysis,” where patients agree to treatments they do not understand simply to alleviate the stress of the encounter.
This is not merely a communication failure; We see a systemic risk. For instance, in the management of Type 2 Diabetes, the “mechanism of action” (how a drug works in the body) for GLP-1 receptor agonists must be clearly communicated to ensure patients manage titration—the gradual increase of a dose—correctly. Without this understanding, the risk of severe gastrointestinal contraindications (reasons why a treatment should not be used) increases, leading to premature discontinuation of life-saving therapy.
Data indicates that health literacy disparities are often mapped directly onto racial and economic lines. According to the World Health Organization (WHO), the inability to access verified health data disproportionately affects marginalized populations, exacerbating the “Inverse Care Law,” which suggests that the availability of decent medical care tends to vary inversely with the need for it in the population served.
Geo-Epidemiological Bridging: From the NHS to the FDA
The approach to treating information as a determinant of health varies significantly by region. In the United Kingdom, the National Health Service (NHS) has begun integrating “Information Prescriptions,” where clinicians prescribe specific, vetted digital resources alongside medication to ensure the patient understands the trajectory of their care.
In the United States, the focus has shifted toward the Centers for Disease Control and Prevention (CDC) “Healthy People 2030” initiative, which aims to move from simply measuring “personal health literacy” to “organizational health literacy.” This means the burden of understanding is shifted from the patient to the healthcare provider; the system must be designed to be understandable to everyone, regardless of education level.
In the Global South, the bridge is being built through mHealth (mobile health). By leveraging high smartphone penetration, researchers are bypassing traditional literacy barriers using audio-visual evidence-based guides. However, the “Digital Divide”—the gap between those with high-speed internet and those without—remains a critical hurdle in achieving true information equity.
“We are fighting a dual battle: the disease itself and the ‘infodemic’ that surrounds it. When quality information is absent, misinformation fills the void, and in medicine, misinformation is a pathogen that spreads faster than any virus.” — Dr. Soumya Swaminathan, former Chief Scientist at the WHO.
Clinical Impact: Health Literacy vs. Patient Outcomes
To understand the gravity of this determinant, we must look at the statistical correlation between information access and clinical stability. The following data summarizes the impact of health literacy on chronic disease management across diverse patient cohorts.
| Literacy Level | Medication Adherence Rate | 30-Day Readmission Risk | HbA1c Control (Diabetes) |
|---|---|---|---|
| Low | 45% – 60% | High (>25%) | Poor (>9%) |
| Moderate | 60% – 80% | Moderate (15-20%) | Fair (7-9%) |
| High | 80% – 95% | Low (<10%) | Good (<7%) |
This research was primarily supported by grants from the National Institutes of Health (NIH) and the Wellcome Trust. Because these are public funding bodies, the research is subject to rigorous peer-review and is free from the commercial bias often found in pharmaceutical-funded trials, ensuring the findings on health equity remain objective.
Contraindications & When to Consult a Doctor
While seeking health information online is a vital part of modern patient autonomy, there are critical “red flags” that indicate you should stop self-researching and seek immediate professional intervention. You must consult a licensed physician if you encounter the following:
- Symptom Overlap: When you find “diagnostic overlap” (where different diseases share the same symptoms), do not attempt to differentiate them via search engines. This often leads to “Cyberchondria” or dangerous self-misdiagnosis.
- Treatment Modification: Never alter the dosage of a prescription medication based on a peer-reviewed study or a health blog. The “N-value” (the number of participants) in a study may be large, but it does not account for your specific comorbidities or genetic contraindications.
- Acute Red Flags: If you experience sudden chest pain, facial drooping, or difficulty breathing, disregard all digital information and call emergency services immediately. Information is a determinant of health, but it is not a replacement for acute clinical triage.
The Future of Medical Intelligence
The recognition of quality information as a fundamental determinant of health marks a paradigm shift in medicine. We are moving away from a paternalistic model—where the doctor holds all the knowledge—toward a collaborative model of “shared decision-making.”
As we integrate AI and large language models into clinical workflows, the risk of “hallucinated” medical data increases. The goal for 2026 and beyond must be the creation of a “Verified Truth Layer” in public health—a global standard of information that is scientifically rigorous, culturally competent, and accessible to the most vulnerable among us. Information is no longer just a tool for the patient; it is the foundation of the cure.
References
- Nature Medicine. (2026). Quality health information for all is a fundamental determinant of health. Doi:10.1038/s41591-026-04320-x
- World Health Organization (WHO). Global Strategy on Digital Health 2020-2025.
- The Lancet. (2025). Health Literacy and the Global Burden of Disease: A Longitudinal Analysis.
- Centers for Disease Control and Prevention (CDC). Healthy People 2030: Health Literacy Framework.