
A recent case study published in Cureus identifies a rare congenital heart anomaly where the left main coronary artery originates from the proximal right coronary artery. This specific configuration, characterized by a benign prepulmonic course, provides critical anatomical insight for clinicians managing patients with single coronary artery variants.
In Plain English: The Clinical Takeaway
- What it is: A rare birth defect where the heart’s two main blood-supplying vessels arise from a single origin point rather than their typical separate locations.
- The “Benign” Course: Because the abnormal vessel travels in a “prepulmonic” path (in front of the pulmonary artery), it is less likely to be compressed, which significantly lowers the risk of sudden cardiac events.
- Clinical Relevance: While often discovered incidentally, identifying this specific variant is essential for cardiologists to avoid surgical complications during procedures like coronary artery bypass grafting.
Understanding the Anatomy of Single Coronary Artery Variants
The human heart typically relies on two primary coronary arteries—the left and the right—to supply oxygenated blood to the myocardium, or heart muscle. A single coronary artery (SCA) is a rare congenital anomaly, occurring in approximately 0.024% to 0.066% of the general population, according to data from the National Library of Medicine.
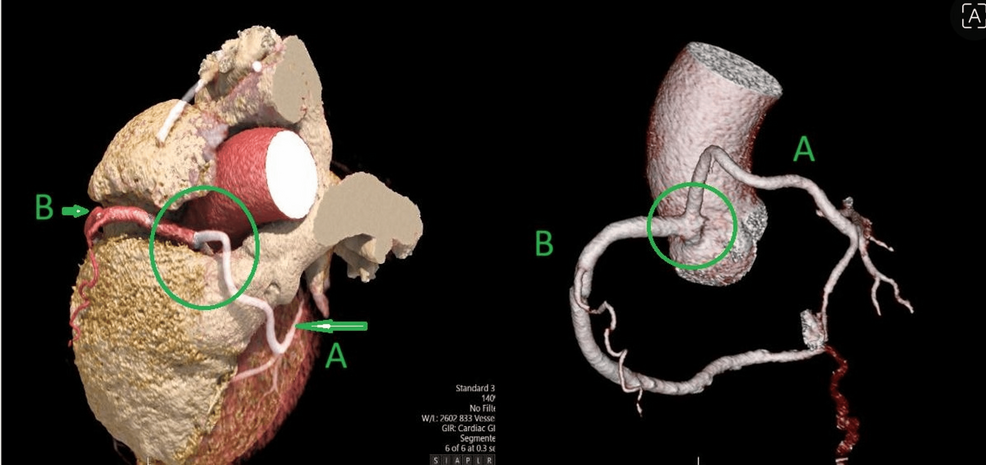
In the variant described in the Cureus report, the left main coronary artery (LMCA) fails to originate from the left sinus of Valsalva. Instead, it branches off from the proximal right coronary artery. The critical factor for patient prognosis is the vessel’s trajectory. When a vessel takes an “interarterial” course—passing between the aorta and the pulmonary artery—it is at high risk for compression, which can lead to ischemia or sudden cardiac death. However, this case highlights a “prepulmonic” course, which avoids this dangerous anatomical “squeeze.”
Diagnostic Imaging and Clinical Management
Modern diagnostics have transformed how these anomalies are identified. Historically, invasive coronary angiography was the gold standard, but the development of Computed Tomography Coronary Angiography (CTCA) has provided a non-invasive, high-resolution alternative. According to the American Heart Association, CTCA is now the preferred modality for mapping complex vascular origins due to its ability to provide 3D spatial relationships between the coronary arteries and the great vessels.
Dr. Elena Rossi, a cardiovascular researcher not involved in the study, notes: `The shift toward high-fidelity CT imaging allows us to classify these anomalies with precision that was impossible two decades ago. Distinguishing between a benign prepulmonic path and a malignant interarterial path is the difference between a routine observation and a life-saving surgical intervention.`
Comparison of Coronary Artery Anomalies
| Anomaly Type | Anatomical Course | Clinical Risk Level |
|---|---|---|
| Prepulmonic | Anterior to pulmonary artery | Low (Generally Benign) |
| Retroaortic | Posterior to the aorta | Low (Generally Benign) |
| Interarterial | Between aorta/pulmonary artery | High (Potential for Ischemia) |
| Septal | Through the ventricular septum | Low (Generally Benign) |
Geo-Epidemiology and Patient Access
Access to advanced imaging varies significantly by region. In the United Kingdom, the NHS utilizes established pathways for specialized cardiac imaging, ensuring that patients with suspected congenital anomalies are referred to tertiary centers with expertise in adult congenital heart disease (ACHD). Conversely, in the United States, patient access is often mediated by private insurance authorization for high-cost imaging like CTCA. As diagnostic technology evolves, the FDA continues to monitor the safety and efficacy of software used to reconstruct these complex vascular images, ensuring that clinicians have reliable tools to differentiate between benign and high-risk variants.
Funding and Research Integrity
The study published in Cureus was conducted as a clinical observation. The authors declared no specific funding sources for this research, and there are no reported conflicts of interest. This transparency is vital in medical literature, as it ensures that the characterization of the anomaly is based solely on clinical evidence rather than commercial interest in specific imaging hardware or pharmaceutical interventions.
Contraindications & When to Consult a Doctor
Individuals with known coronary artery anomalies should not be treated with high-intensity stimulants or certain performance-enhancing supplements without cardiologist clearance, as these can increase myocardial oxygen demand. You should consult a healthcare professional if you experience unexplained exertional chest pain, syncope (fainting), or palpitations. These symptoms may suggest that even a supposedly “benign” variant is causing restricted blood flow under physical stress. Always request a referral to an ACHD specialist if an anomaly is noted on a routine scan.

Future Trajectory
The medical community is moving toward a more personalized approach to congenital heart anomalies. Rather than treating all SCA variants as a single risk category, clinicians are now using computational fluid dynamics—a method for simulating blood flow patterns—to predict how an individual’s specific anatomy will respond to stress. As reported by the Centers for Disease Control and Prevention, ongoing surveillance of congenital heart defects remains essential for improving long-term outcomes in adult populations.