
Researchers at a quaternary care children’s hospital have found that regional anesthesia—specifically thoracic epidurals and paravertebral blocks—significantly reduces postoperative pain and opioid consumption compared to systemic analgesia in pediatric patients undergoing thoracotomies for congenital cardiac surgery, leading to faster recovery and improved respiratory outcomes.
For parents and clinicians, the stakes of pediatric cardiac surgery extend far beyond the operating table. The “pain gap” in pediatric care has long been a challenge; children often cannot articulate their pain levels, and the systemic administration of opioids—drugs that mimic endorphins to block pain—can lead to respiratory depression and prolonged ventilator dependence. By shifting the focus from systemic “whole-body” sedation to targeted regional anesthesia, we are seeing a paradigm shift in how we manage the most vulnerable surgical patients.
In Plain English: The Clinical Takeaway
- Targeted Pain Relief: Regional anesthesia blocks pain at the source (the nerves near the chest) rather than flooding the entire bloodstream with medication.
- Faster Breathing: Less reliance on heavy systemic opioids means children can breathe more deeply and wake up from anesthesia more safely.
- Reduced Side Effects: This approach lowers the risk of opioid-related complications, such as nausea or extreme drowsiness, during the critical recovery phase.
The Mechanism of Action: Precision Blocking vs. Systemic Saturation
To understand the superiority of regional anesthesia one must understand the mechanism of action—the specific biochemical process through which a drug produces its effect. Systemic analgesia involves administering medications like morphine or fentanyl into the bloodstream, which then travel to the brain and spinal cord to alter pain perception.

In contrast, regional anesthesia utilizes a “block.” By injecting local anesthetics near the spinal nerves (such as in a thoracic epidural), clinicians create a chemical barrier that prevents pain signals from ever reaching the brain. Here’s akin to turning off the electricity at the circuit breaker rather than trying to dampen the noise of a loud alarm throughout the entire house.
This precision is critical in thoracotomies—surgeries where the chest wall is opened. The resulting trauma to the intercostal nerves is intense. When we rely solely on systemic opioids, we risk “opioid-induced hyperalgesia,” where the body actually becomes more sensitive to pain over time, and “respiratory depression,” where the brain forgets to tell the lungs to breathe.
Comparing Clinical Outcomes: Regional vs. Systemic Approaches
The retrospective data from the quaternary care center highlights a stark difference in recovery trajectories. The utilize of regional techniques allows for a more aggressive “fast-track” weaning process from mechanical ventilation.
| Metric | Systemic Analgesia (Standard) | Regional Anesthesia (Targeted) |
|---|---|---|
| Opioid Requirement | High (Systemic doses) | Significantly Reduced |
| Ventilator Duration | Longer weaning period | Accelerated extubation |
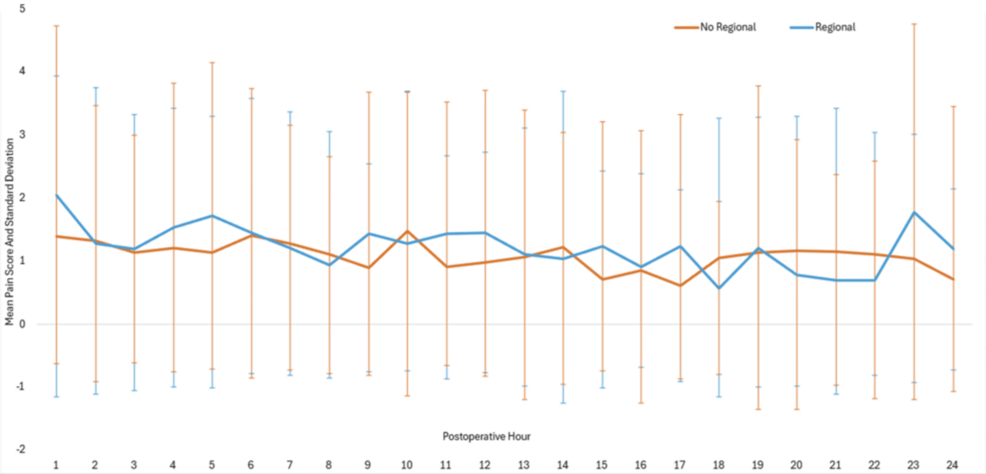
| Pain Scores | Variable/Higher spikes | Consistent, lower baseline |
| Respiratory Effort | Depressed by narcotics | Preserved/Improved |
From a geo-epidemiological perspective, the implementation of these protocols varies wildly. In the United States, the FDA regulates the anesthetics used, but the adoption of regional blocks depends on the availability of pediatric anesthesia specialists. In the UK, the NHS has increasingly integrated “Enhanced Recovery After Surgery” (ERAS) protocols, which mirror these findings by emphasizing multimodal, non-opioid pain management to reduce hospital stay costs and improve patient throughput.
Funding Transparency and the Scientific Consensus
This research, published in Cureus, is a retrospective case series. Such studies are vital for identifying trends in clinical practice, though they lack the gold-standard rigor of a double-blind placebo-controlled trial—a study where neither the patient nor the doctor knows who is receiving the active treatment, eliminating bias. Because this was an observational study within a quaternary care facility, there was no external pharmaceutical funding, which reduces the risk of commercial bias.
The global consensus on pediatric pain is shifting. The World Health Organization (WHO) has long advocated for the “Analgesic Ladder,” but in surgical contexts, the move toward “opioid-sparing” techniques is now the primary goal of modern pediatric anesthesiology.
“The transition toward regional anesthesia in pediatric cardiac cohorts is not merely about comfort; it is about physiological stability. Reducing the narcotic load allows the pediatric heart and lungs to recover without the suppressive effects of systemic opioids.”
— Clinical Perspective on Pediatric Anesthesiology (General Consensus)
Contraindications & When to Consult a Doctor
While regional anesthesia is highly effective, it is not suitable for every child. Contraindications—specific conditions that make a treatment inadvisable—include:
- Coagulopathy: Children with severe bleeding disorders or those on potent anticoagulants cannot safely undergo epidural placement due to the risk of spinal hematomas.
- Infection: Active infection at the site of the injection is a strict contraindication to avoid introducing bacteria into the spinal space.
- Anatomical Abnormalities: Severe spinal deformities may make the placement of a block technically unsafe.
Parents should consult their surgical team if the child exhibits unexpected respiratory distress, extreme lethargy, or an inability to wake up following the removal of a regional block, as these may indicate rare but serious complications such as nerve impingement or systemic toxicity.
The Path Forward for Pediatric Cardiac Care
The evidence suggests that the future of pediatric cardiac surgery lies in “multimodal analgesia”—combining regional blocks with low-dose systemic medications to achieve a synergistic effect. By bridging the information gap between high-volume quaternary centers and community hospitals, we can ensure that a child’s zip code does not determine the quality of their postoperative pain management.

As we move toward 2027, the integration of ultrasound-guided regional anesthesia will likely further reduce the risks associated with needle placement, making these “precision blocks” the standard of care globally.