
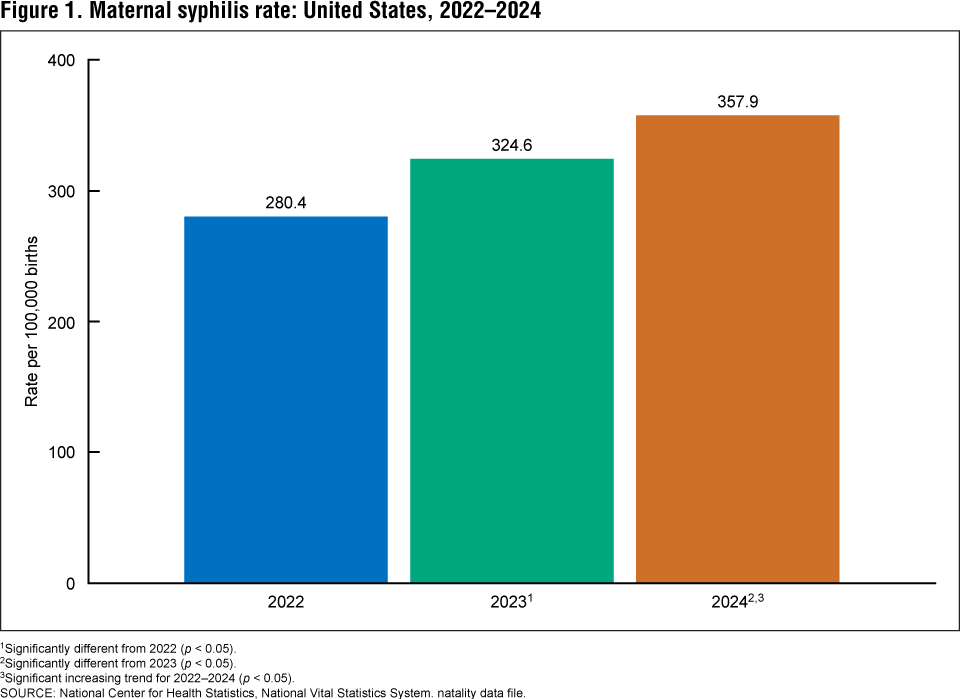
In 2024, syphilis rates among pregnant women in the United States reached 887 cases per 100,000 births for Black women, 411 for Hispanic women, and 2,145 for Native American and Alaskan Native women, according to the National Center for Health Statistics. This represents a 222% increase from 2016 to 2022 and a further 28% rise from 2022 to 2024, driven largely by gaps in prenatal screening and treatment access. Congenital syphilis, which can cause stillbirth, neonatal death, and lifelong disability, is preventable with timely penicillin-based treatment, yet systemic barriers in underserved communities continue to fuel the epidemic.
Why Rising Maternal Syphilis Demands Urgent Public Health Action
The resurgence of congenital syphilis is not merely a clinical concern but a stark indicator of failing maternal healthcare infrastructure. When a pregnant person tests positive for syphilis, a single intramuscular dose of benzathine penicillin G — the only antibiotic proven to cross the placenta and treat fetal infection — can prevent transmission if administered at least 30 days before delivery. However, delays in diagnosis, especially among those without consistent prenatal care, allow the spirochete Treponema pallidum to invade fetal tissues, causing multisystem damage. The CDC estimates that 9 in 10 congenital syphilis cases could be averted with timely screening and treatment, yet 40% of affected mothers in 2022 received no or inadequate prenatal care. This gap reflects not individual failure but structural inequities: insurance gaps, clinic closures in rural areas, and transportation barriers disproportionately impact low-income individuals and people of color.
In Plain English: The Clinical Takeaway
- Syphilis in pregnancy is treatable with penicillin, but only if detected early through routine blood tests.
- Skipping prenatal care increases the risk of undiagnosed syphilis, which can lead to miscarriage, stillbirth, or severe birth defects.
- Expanding access to testing — especially in underserved communities — is the most effective way to stop preventable infant harm.
Geographic and Systemic Drivers of Disparity
The burden of maternal syphilis is unevenly distributed, with Native American and Alaskan Native populations experiencing rates over 11 times higher than white women (2,145 vs. 188.2 per 100,000 births). These disparities correlate with long-standing underfunding of Indian Health Service (IHS) facilities, many of which lack obstetric specialists or consistent laboratory capacity for syphilis screening. In contrast, states with mandatory third-trimester and delivery-screening policies — such as California and New York — have seen slower growth in congenital cases, though even these regions report increases among unhoused and uninsured populations. The Indian Health Service, a federally funded program under the Department of Health and Human Services, serves approximately 2.6 million Native Americans but operates under chronic budget constraints that limit prenatal outreach. Meanwhile, the Centers for Disease Control and Prevention’s Division of STD Prevention allocates annual grants to state health departments for syphilis outreach, yet funding levels have not kept pace with rising case volumes, according to a 2023 Government Accountability Office review.
Evidence Behind the Prevention Strategy
The effectiveness of penicillin in preventing congenital syphilis is grounded in decades of clinical observation and pharmacologic research. Benzathine penicillin G, a long-acting intramuscular formulation, maintains treponemicidal levels in maternal blood for up to four weeks, ensuring sustained exposure to the fetus. A 2022 randomized controlled trial published in The Lancet Infectious Diseases confirmed that a single 2.4 million unit dose achieves adequate treponemacidal activity in pregnant women with early syphilis, matching the efficacy of the traditional three-dose regimen. This finding supports updated World Health Organization guidelines recommending single-dose benzathine penicillin G for maternal syphilis treatment where adherence to multi-dose regimens is challenging. Crucially, no alternative antibiotic has demonstrated reliable placental penetration or fetal efficacy; doxycycline and azithromycin are contraindicated in pregnancy due to risks of tooth discoloration and antimicrobial resistance, respectively.
“We have the tools to eliminate congenital syphilis — a safe, inexpensive, and highly effective treatment exists. What we lack is the political will to ensure every pregnant person, regardless of zip code or income, receives timely testing, and care.”
— Dr. Leandro Mena, Director, Division of STD Prevention, Centers for Disease Control and Prevention, Statement to Congress, March 2024
Closing the Gap: Policy and Access Solutions
Addressing this crisis requires aligning clinical practice with equity-focused public health policy. The American College of Obstetricians and Gynecologists now recommends triple screening — at first prenatal visit, 28–32 weeks, and delivery — a shift endorsed by the U.S. Preventive Services Task Force in 2023. Implementation, however, depends on state Medicaid programs covering these additional tests and clinics having the staff to administer them. In 2023, the Health Resources and Services Administration awarded $60 million in grants to expand maternal health access in underserved areas, including funding for mobile clinics and telehealth obstetrics. Yet, as of early 2026, fewer than 40% of eligible rural clinics have adopted point-of-care syphilis testing, which delivers results in under 15 minutes and could significantly increase same-day treatment initiation. Experts emphasize that stigma remains a barrier; many individuals avoid testing due to fear of judgment or legal repercussions, particularly in states with punitive policies around substance use or sexual health.
Contraindications & When to Consult a Doctor
All pregnant individuals should be screened for syphilis regardless of symptoms, as early infection is often asymptomatic. Those who test positive must receive benzathine penicillin G unless they have a documented history of severe allergy (e.g., anaphylaxis) to penicillin, in which case desensitization protocols under specialist supervision are required — there is no safe alternative for fetal treatment. Anyone experiencing a painless sore (chancre), rash on palms or soles, fever, or swollen lymph nodes should seek testing immediately, though absence of symptoms does not rule out infection. Prompt treatment not only protects the fetus but also reduces the mother’s risk of neurosyphilis or cardiovascular complications years later.
The Path Forward: Elimination Is Possible
Cuba validated the World Health Organization’s dual elimination goal for mother-to-child transmission of HIV and syphilis in 2015 through universal access to prenatal care, rapid testing, and stockpiled penicillin. The United States, despite its vast resources, has yet to achieve this benchmark due to fragmented healthcare delivery and persistent inequities. However, models from states like Connecticut — which combined Medicaid expansion, provider education, and community-based outreach to reduce congenital syphilis by 40% between 2020 and 2023 — demonstrate that progress is possible when systems prioritize reach over rhetoric. As of February 2026, the CDC’s Syphilis Elimination Campaign continues to partner with community health centers to distribute free test kits and train non-clinical staff in outreach, recognizing that ending this epidemic requires meeting people where they are: in clinics, jails, shelters, and on the streets.
References
- National Center for Health Statistics. (2024). Maternal syphilis rates, 2016–2024. CDC.
- Centers for Disease Control and Prevention. (2023). Sexually Transmitted Disease Surveillance 2022.
- World Health Organization. (2022). Global guidance on the validation of elimination of mother-to-child transmission of HIV and syphilis.
- Ladner, J. Et al. (2022). Single-dose benzathine penicillin G for early syphilis in pregnancy: A randomized controlled trial. The Lancet Infectious Diseases, 22(5), 678–686. doi:10.1016/S1473-3099(22)00123-4
- U.S. Preventive Services Task Force. (2023). Screening for syphilis in pregnancy: Recommendation statement.